Article Content
Abstract
Background
Lip and oral cavity cancer is a significant global health concern, with increasing incidence rates in recent years. Understanding epidemiological trends and their associated risk factors is crucial for effective prevention and management.
Aim
This study aimed to analyze global, regional, and national trends in lip and oral cavity cancer incidence, mortality, and disability-adjusted life-years (DALYs) from 1990 to 2021 to assess key risk factors and sociodemographic influences to support clinical pharmacy interventions and improve patient outcomes.
Method
Lip and oral cavity cancer burden was analyzed by location, age, and sex. Joinpoint regression assessed trends, Spearman correlation measured sociodemographic index (SDI) associations, and decomposition analysis quantified population growth, aging, and epidemiological impacts. Cross-country disparities and risk factors were also evaluated.
Results
In 2021, there were 421,577 (95% uncertainty interval [UI]: 389,879–449,782) new lip and oral cavity cancer cases, 208,379 (95% UI: 191,288–224,162) deaths, and 5,874,070 (95% UI: 5,326,986–6,347,557) DALYs globally, with the highest burden in South Asia. The age-standardized incidence rate (ASIR) increased significantly, while the age-standardized mortality rate (ASMR) and age-standardized DALYs rate slightly declined. Men and older adults had higher rates, but the increase was more pronounced in women and younger populations. ASIR correlated positively with SDI, while cross-country inequalities persisted, particularly in low-SDI regions. The contribution of tobacco chewing to lip and oral cavity cancer deaths and DALYs slightly increased.
Conclusion
The incidence of lip and oral cavity cancer continues to increase, with a shifting burden on younger individuals and women. Targeted interventions to reduce risk factors and improve access to healthcare are essential for high-risk populations and regions.
Explore related subjects
Discover the latest articles and news from researchers in related subjects, suggested using machine learning.
- Cancer Epidemiology
- Dental epidemiology
- Head and Neck Cancer
- Oral Cancer Detection
- Oral Cancer
- Oral Diseases
Impact statements
- The increasing incidence of lip and oral cavity cancer among younger populations and women necessitates age- and sex-specific prevention strategies, including enhanced screening programs and education on emerging risk factors, such as HPV infection and smokeless tobacco use.
- The significantly higher burden in South Asia and low-SDI countries demonstrates the need for region-specific strategies including improved healthcare accessibility, stronger tobacco control policies, and pharmacist-led interventions for early detection and patient support.
- With population growth and aging as major contributors to increasing lip and oral cavity cancer DALYs, healthcare systems must strengthen multidisciplinary approaches, including pharmacist-led supportive care, pain management, and treatment adherence strategies to improve patient outcomes.
Introduction
Lip and oral cavity cancer is a prevalent malignancy of the head and neck, characterized by aggressive progression and poor prognosis, with a five-year survival rate of approximately 50% [1, 2]. Surgical resection remains the primary treatment approach; however, extensive surgical procedures often lead to significant functional impairments, including dysphagia, speech deficits, and loss of taste and olfactory function, profoundly affecting patients’ psychological well-being, physical health, and overall quality of life [3].
These complications highlight the importance of multidisciplinary care in which clinical pharmacists play a key role in cancer care. They use tools like the Pharmaceutical Care Network Europe (PCNE) classification to address drug-related problems (DRPs), optimize chemotherapy and pain management, minimize medication errors, and manage side effects. Clinical pharmacists also contribute to multidisciplinary team (MDT) to improve resource allocation and reduce costs. Using digital tools like mobile health apps, they can remotely monitor pain and provide personalized interventions [4,5,6]. The role of clinical pharmacists in integrated cancer care will continue to grow.
The global incidence of lip and oral cavity cancer has steadily increased. According to GLOBOCAN data, approximately 377,000 new cases and 177,000 deaths were reported worldwide in 2020 [7]. The burden is particularly pronounced in low- and middle-income countries, where lip and oral cavity cancer ranks as the fourth most common malignancy and the sixth leading cause of cancer-related mortality [8]. The increasing prevalence of risk factors such as tobacco use, excessive alcohol consumption, betel quid chewing, and human papillomavirus (HPV) infection has further exacerbated this global health challenge [9,10,11]. Additionally, aging populations contribute to an increasing disease burden, necessitating comprehensive prevention and early intervention strategies [12].
Previous studies have estimated global incidence and mortality trends based on earlier versions of the Global Burden of Disease (GBD) Study and GLOBOCAN data [7, 13,14,15,16], and Sun et al. further explored temporal changes in attributable risk factors of lip and oral cavity cancer[17]. However, a critical gap remains in research analyzing the key drivers of the rising disease burden and quantifying cross-country health inequalities using appropriate metrics. Although recent analyses using the GBD 2021 database have provided valuable insights into lip and oral cavity cancer burden in China and India [18, 19], they lack a comprehensive global perspective on trends and risk factor attributions. A deeper understanding of these trends is essential for guiding clinical decision-making, optimizing pharmacological interventions, and informing public health policies to reduce the burden of lip and oral cavity cancer.
Aim
This study aimed to analyze global, regional, and national trends in the incidence, mortality, and disability-adjusted life-years (DALYs) of lip and oral cavity cancer from 1990 to 2021 using the latest GBD 2021 dataset while assessing key risk factors and sociodemographic influences to provide evidence for optimizing clinical pharmacy interventions and improving patient outcomes.
Ethics approval
This study did not require ethics approval as it utilized publicly available, de-identified data from the GBD 2021 database.
Method
Data sources
The GBD 2021 dataset encompasses estimates of 371 diseases and injuries and 88 risk factors across 21 regions and 204 countries/territories from 1990 to 2021, including lip and oral cavity cancer. The GBD database employed spatiotemporal Gaussian process regression (ST-GPR) to address data gaps in regions with incomplete datasets and utilized, Bayesian meta-regression (DisMod-MR 2.1) to ensure internally consistent estimates. Detailed methods for data collection, processing, and analysis are available in the GBD 2021 capstone reports [20, 21].
This study analyzed lip and oral cavity cancer incidence, mortality, and DALYs in absolute counts and age-standardized rate (ASR) per 100,000 population, stratified by sex and age. Given the rarity of lip and oral cavity cancer in children [22] and the absence of data for the 0–15 age group in GBD 2021, our analysis focused on individuals aged 15–95 + years, with subgroups of five-year intervals (15–19 to 95 + years). Data were extracted from the Global Health Data Exchange GBD Results Tool (https://vizhub.healthdata.org/gbd-results/). Additionally, the sociodemographic index (SDI), a composite measure of income, education, and fertility, was included to examine variations across five SDI quintiles: high, high-middle, middle, low-middle, and low [20]. This study followed the Guidelines for Accurate and Transparent Health Estimates Reporting (GATHER) [23].
Definition of lip and oral cavity cancer
The GBD 2021 defines lip and oral cavity cancer based on the International Classification of Diseases, Tenth Revision (ICD-10) codes C00 to C08 [20].
Statistical analyses
Descriptive and trend analyses
The lip and oral cavity cancer burden was analyzed at the global, regional, and national levels, as well as across SDI quintiles. The age-standardized incidence rate (ASIR), age-standardized mortality rate (ASMR), and age-standardized DALYs rate were reported per 100,000 population using the GBD 2021 world population standard [20].
Analyzing disease burden trends is vital in epidemiology for developing targeted prevention strategies. Temporal trends from 1990 to 2021 were assessed using the average annual percent change (AAPC) via Joinpoint regression analysis. This software uses the grid search method (GSM) and Monte Carlo permutation test to detect joinpoints, estimate parameters, and select optimal models. Specifically, the GSM divides the data into multiple grids, calculates the sum of squared errors (SSE) and mean squared error (MSE) for each potential scenario, and selects the grid point with the minimum MSE as the optimal joinpoint. Subsequently, the Monte Carlo permutation test validates the final model by statistically determining the optimal number of joinpoints (as detailed in Supplementary Method) [24]. The trends in the ASIR, ASMR, and age-standardized DALYs rate were quantified using AAPC from the optimal model. AAPC values above or below zero indicate increasing or decreasing trends, respectively, while values near zero suggest stability. Model fit was tested through residual analysis, with an average relative error ≤ 10% indicating a satisfactory fit [25]. To assess the robustness of findings and account for data fluctuations, a sensitivity analysis was performed using the lower and upper data bounds.
Correlation between ASR and SDI
To evaluate the relationship between the SDI and lip and oral cavity cancer burden across countries, Spearman’s correlation analysis was conducted. Spearman’s rank correlation coefficient (ρ) measures the strength and direction of the association, ranging from − 1 to + 1, with a significance level of p < 0.05 indicating a statistically significant correlation.
Decomposition analysis
To identify the key contributors to changes in lip and oral cavity cancer DALYs from 1990 to 2021, decomposition analysis was performed using Das Gupta’s method [26]. This approach isolates the contributions of population growth, aging, and epidemiological shifts to variations in DALYs, with positive and negative contributions indicating increases and decreases in disease burden, respectively.
Attributable risk factors
In addition to incidence and mortality, this study assessed the proportion of lip and oral cavity cancer burden attributable to major risk factors, including smoking, chewing tobacco, and alcohol use, as identified in the GBD 2021. These risk-exposure pairs were selected based on the criteria of the World Cancer Research Fund for convincing or probable evidence. The lowest theoretical risk exposure was defined as lifelong non-use of smoking and chewing tobacco and alcohol consumption of 0–10 g/day [13]. Temporal trends in risk factor contributions from 1990 to 2021 were analyzed using AAPC.
Cross-country analysis of inequalities
Monitoring health inequalities provides a basis for evidence-based health planning and further facilitates the development of equitable and effective health policies to reduce such inequalities [27]. To assess disparities in lip and oral cavity cancer burden across countries, the concentration index recommended by the World Health Organization (WHO) was used as a measure of relative inequality [28]. The concentration index was calculated by integrating the Lorenz concentration curve and plotting cumulative DALYs against the cumulative relative distribution of populations ranked by SDI [29]. The values range from − 1 to + 1, with positive values indicating a concentration of burden in high-SDI countries and negative values indicating a concentration in low-SDI countries. A value approaching 0 suggests minimal inequality, while a value close to 0.2 is considered indicative of significant health inequity [28].
Software and statistical tools
All statistical analyses and visualizations were conducted using R (version 4.4.1) and Joinpoint regression software (version 5.2.0).
Results
Global trends in lip and oral cavity cancer burden
From 1990 to 2021, the global number of lip and oral cavity cancer incidence, deaths, and DALYs increased by 142.18%, 113.94%, and 100.06%, respectively. ASIR exhibited an increasing trend (AAPC: 0.44%), whereas ASMR and age-standardized DALYs rate showed slight declines (AAPC: − 0.03% and − 0.07%, respectively) (Tables 1, 2, 3).
Regionally, South Asia reported the highest ASIR, ASMR, and age-standardized DALYs rate, whereas Oceania had the lowest number of cases. The lowest ASIR was observed in Western Sub-Saharan Africa, whereas North Africa and Middle East recorded the lowest ASMR and age-standardized DALYs rate. The largest increase in ASIR occurred in East Asia, whereas Western Sub-Saharan Africa had the highest growth in ASMR and age-standardized DALYs rate. In contrast, the greatest decline in ASIR was observed in High-income North America, whereas Western Europe experienced the largest reductions in ASMR and age-standardized DALYs rate (Tables 1, 2, 3).
At the national level, India had the highest incidence, mortality, and DALYs burden in 2021, followed by China, whereas Tokelau had the lowest. The highest ASIR, ASMR, and age-standardized DALYs rate values were reported in Palau, whereas the lowest were found in São Tomé and Príncipe. From 1990 to 2021, Cabo Verde showed the most significant increase in ASIR, ASMR, and age-standardized DALYs rate, whereas Kuwait experienced the largest decline (Supplementary Tables 1, 2, and 3).
According to the SDI classification, the highest incidence in 2021 was observed in the middle SDI group, whereas mortality and DALYs were the highest in the low-middle SDI group. The lowest values across all three measures were recorded in the low-SDI group. Notably, ASIR was highest in the low-middle SDI, whereas ASMR and age-standardized DALYs rate were highest in the same SDI category. The middle SDI showed the largest increase in ASIR, while the low-middle SDI showed the greatest increase in ASMR and age-standardized DALYs rate. Conversely, the high SDI group exhibited the largest decline in all three metrics (Tables 1, 2, 3).
The residual analysis confirmed an excellent model fit, with average relative error values consistently < 10.00% (Supplementary Table 4). An example of the detailed model selection process was provided in Supplementary Table 5. Additionally, the results of sensitivity analyses showed similar trends when modeling data lower/upper bounds (Supplementary Tables 6). These results further demonstrated the reliability and stability of trend analysis methods.
Sex- and age-specific trends
Between 1990 and 2021, the incidence, death, and DALYs of lip and oral cavity cancer have increased in both men and women. While men consistently exhibited higher ASIR, ASMR, and age-standardized DALYs rate than women, the increase in ASIR was more pronounced in women (AAPC: 0.78%) than in men (AAPC: 0.26%) (Table 1). Meanwhile, ASMR and age-standardized DALYs rate declined in men (AAPC: − 0.18% and − 0.22%, respectively) but increased in women (AAPC: 0.26% and 0.24%, respectively) (Tables 2, 3).
Age-wise, the highest number of incident and fatal cases was observed in the 65–69 age group, while DALYs peaked in the 55–59 age group (Supplementary Fig. 1). The highest ASIR was found in individuals aged 90–94 years, whereas ASMR and age-standardized DALYs rate peaked in individuals aged 95 years and above. Between 1990 and 2021, the ASIR, ASMR, and age-standardized DALYs rate increased in individuals younger than 44 years, with the highest AAPC in the 20–24 age group. The ASIR increased in all age subgroups except for the 50–54 age group, while ASMR and age-standardized DALYs rate declined significantly in individuals aged 45–69 years, particularly in the 50–54 age group (Fig. 1; Supplementary Table 7).
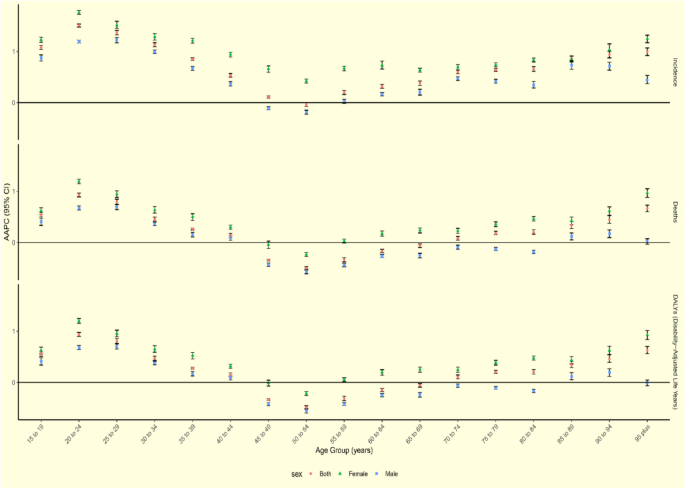
The global AAPC of incidence, deaths, and DALYs for lip and oral cavity cancer from 1990 to 2021 by age group and sex. Abbreviations: AAPC, average annual percentage change; DALYs, disability-adjusted life-years
Men had higher incidence and mortality rates in most age groups (Supplementary Fig. 1). However, in the 15–19, 20–24, 90–94, and 95-plus age subgroups, women had more cases and higher ASIR, ASMR, and age-standardized DALYs rate. Additionally, women in all age groups demonstrated a steeper upward trend in ASIR, ASMR, and age-standardized DALYs rate than men, with the highest AAPC observed in women aged 20–24 years and men aged 25–29 years (Fig. 1; Supplementary Table 7).
Association between SDI and lip and oral cavity cancer burden
A significant positive correlation was observed between SDI and ASIR (ρ = 0.44, P < 0.001), indicating that regions with higher SDI had higher incidence rates of lip and oral cavity cancer (Supplementary Fig. 2). However, the correlations between the SDI and ASMR (ρ = − 0.08, P = 0.261) and between the SDI and age-standardized DALYs rate (ρ = − 0.08, P = 0.266) were not statistically significant.
Decomposition analysis
Between 1990 and 2021, DALYs due to lip and oral cavity cancer have increased globally, with the highest growth occurring in the low-middle SDI group (Supplementary Fig. 3). Population growth was the primary driver, contributing 70.75% to the increase in DALYs, followed by aging (32.85%), whereas epidemiological change contributed -3.59%, indicating a reduction in DALYs due to improved healthcare (Supplementary Table 8). The high SDI group showed the most significant impact of aging (97.50%) and population growth (107.95%), whereas the low-middle SDI group showed the largest epidemiological change effect (7.72%). The epidemiological shift had a net negative effect on DALYs in the high SDI (− 105.45%) and high-middle SDI (− 69.76%) groups. When stratified by sex, the demographic effects were similar, but the epidemiological effects were globally negative for men and positive for women (Supplementary Fig. 3).
Cross-country inequality analysis
The burden of lip and oral cavity cancer exhibited increasing disparities across SDI levels from 1990 to 2021 (Fig. 2). The age-standardized DALYs rate was disproportionately concentrated in low-SDI countries. The concentration index, reflecting relative health inequality, increased from − 0.19 (95% CI − 0.25 to − 0.13) in 1990 to − 0.23 (95% CI − 0.30 to − 0.15) in 2021, demonstrating a worsening trend in global health disparities.
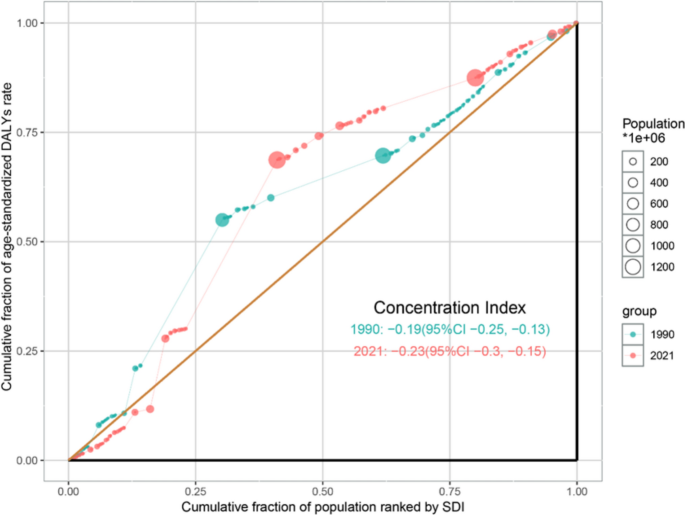
SDI-related health inequality concentration curves for the age-standardized DALYs rate of lip and oral cavity cancer globally, comparing 1990 and 2021. Abbreviations: DALYs, disability-adjusted life-years; SDI, socio-demographic index
Risk factor contributions
Between 1990 and 2021, the contribution of smoking and alcohol use to lip and oral cavity cancer deaths and DALYs declined, whereas tobacco chewing showed a slight increase (Supplementary Fig. 4). In 2021, smoking has remained the leading risk factor for lip and oral cavity cancer, although its impact has decreased globally. Smoking contributed the most in the high-middle SDI regions, alcohol use in the high SDI regions, and chewing tobacco in the low-middle SDI regions. In the high and high-middle SDI groups, chewing tobacco accounted for less than 3% of lip and oral cavity cancer deaths and DALYs, whereas its impact was substantially higher in the other SDI categories.
Regionally, smoking contributed the most to the lip and oral cavity cancer burden in East Asia, alcohol use in Central Europe, and tobacco chewing in South Asia. The impact of smoking declined across most regions except East Asia, while alcohol use remained the predominant risk factor in Australasia, Central Europe, Southern Latin America, and Western Europe. Chewing tobacco contributed to less than 10% of the burden in most regions, except in South and Southeast Asia (Supplementary Fig. 4).
Age-stratified analysis showed that the contribution of all risk factors increased the most in the 25–29 age group from 1990 to 2021, whereas the largest decline was observed in the 50–54 age group (Fig. 3; Supplementary Tables 9 and 10). The impact of smoking decreased in both sexes, with a more significant decline observed in women. Alcohol use declined in most female age groups, with the sharpest reduction observed in those aged 50–54 years. In contrast, alcohol use increased among men aged < 39 years, peaking in the 25–29 age group. The impact of chewing tobacco increased, particularly among women aged 55 years and older, whereas in men, the highest increase was observed in the 40–44 age group. Temporal trends in risk factor contributions to lip and oral cavity cancer ASMR and age-standardized DALYs rate across age groups were presented in Supplementary Fig. 5–8 and 9–12, respectively.
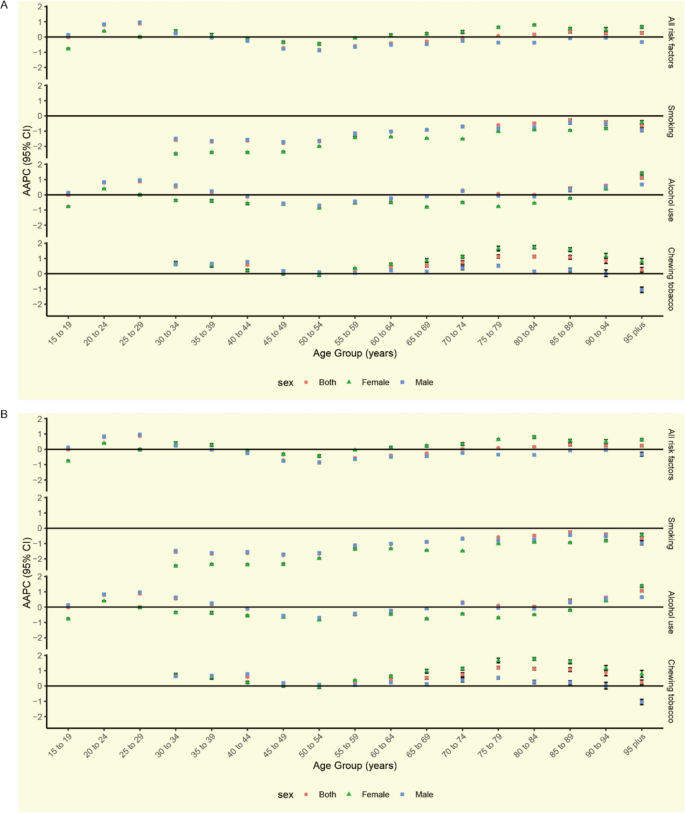
AAPC of lip and oral cavity cancer ASMR (A) and age-standardized DALYs rate (B) attributable to each risk factor from 1990 to 2021 by age group and sex. Abbreviations: AAPC, average annual percent change; ASMR, age-standardized mortality rate; DALYs, disability-adjusted life-years
Discussion
Lip and oral cavity cancer remains a significant global health concern, with an increasing incidence despite advances in early detection and treatment. This study provides a comprehensive analysis of lip and oral cavity cancer burden from 1990 to 2021, highlighting trends across different regions, age groups, and socioeconomic levels. These findings emphasize the urgent need for targeted prevention, improved screening programs, and equitable healthcare access.
Global trends and contributing factors
The ASIR of lip and oral cavity cancer has increased significantly (AAPC: 0.44%), primarily due to population growth, aging, and changing lifestyle factors. Advances in diagnostic methods such as artificial intelligence-assisted screening and salivary biomarkers have improved early detection [30,31,32,33]. The WHO’s Global Strategy for Oral Health (2023–2030) reinforces the need to integrate lip and oral cavity cancer prevention into public health initiatives [34,35,36]. Despite improved treatment approaches, mortality and DALYs have declined only slightly, highlighting the need for more accessible and effective therapies. Clinical pharmacists play an essential role in managing treatment regimens, minimizing drug reactions, improving patient compliance, and individualizing treatment for special populations.
Geographic and socioeconomic disparities
Significant regional differences exist in the lip and oral cavity cancer burden. South Asia, particularly India, has the highest incidence owing to widespread tobacco and betel quid use, along with socioeconomic barriers limiting healthcare access [18, 37, 38]. China has a rapidly increasing burden owing to smoking, alcohol use, and HPV infections [39,40,41]. Meanwhile, high-income North America reports a high incidence but lower mortality, largely due to superior healthcare infrastructure and early detection programs [42]. The growing burden in low-income and middle-income countries demonstrates the need for improved public health policies and equitable access to care.
Increasing incidence among younger populations
This study confirms a concerning increase in lip and oral cavity cancer cases among younger individuals, particularly among individuals under 44 years old. The increasing role of HPV, particularly HPV-16, is evident among younger patients without traditional risk factors, such as smoking and alcohol use [43]. While tobacco control efforts have led to reduced smoking rates, the rising consumption of smokeless tobacco products remains an underregulated challenge [44,45,46]. These trends call for expanded HPV vaccination programs, targeted risk-reduction efforts, and improved screening strategies for younger populations.
Sex-based differences in lip and oral cavity cancer burden
Men consistently show higher ASIR, ASMR, and age-standardized DALY rates than women, primarily due to greater exposure to known risk factors such as smoking and alcohol consumption [47,48,49,50]. However, our study found that women aged 15–24 now had a higher incidence rate than men, reflecting increased smoking and alcohol use among women and potential hormonal influences on cancer progression [50, 51]. These findings emphasize the need for sex-specific prevention and treatment approaches.
Impact of population growth and aging
Our decomposition analysis revealed that population growth (70.75%) and aging (32.85%) were the primary contributors to increasing DALYs, while epidemiological changes had a mitigating effect (-3.59%). The high-SDI regions experienced the strongest effects of aging, whereas the low-middle SDI regions showed an increase in DALYs due to worsening epidemiological trends. As the global population ages, clinical pharmacists play a key role in managing polypharmacy and optimizing therapy for older patients with cancer.
Health inequalities and access to care
This study confirms that the lip and oral cavity cancer burden is increasingly concentrated in lower-income regions, where healthcare access is limited. The highest ASMR and age-standardized DALY rates were observed in the low-middle SDI areas, and the concentration index analysis revealed worsening disparities over time. Expanding preventive programs, improving access to early detection, and implementing resource-appropriate pharmacotherapy interventions are critical for addressing these inequalities.
Shifting risk tactor contributions
While smoking remains the leading risk factor for lip and oral cavity cancer, its contribution has declined in most regions except East Asia. Alcohol use continues to be a major contributor, particularly in high-income countries, while chewing tobacco remains a significant risk factor in South and Southeast Asia [44, 45, 52]. The highest impact of risk factors was observed in the 25–29 age group, emphasizing the need for continued monitoring of emerging risk behaviors. Pharmacists can support prevention efforts by modifiable risk factors such as smoking and alcohol consumption, educating patients, and promoting policy-driven public health initiatives. For smoking, pharmacists offer cessation guidance, recommend medications, conduct motivational interviews, and follow up to help patients quit [53]. For alcohol, they treat it as a “drug” affecting treatment, assess its impact on drug efficacy and safety, remind patients of risks, refer those with drinking problems, and reduce alcohol-related lip and oral cavity cancer risks [54].
Limitations
This study has several limitations. Variations in data quality across countries may affect the burden estimates. Additionally, key risk factors, such as HPV, were not included in the GBD dataset because of insufficient global evidence. Finally, the lack of histopathological and staging data limits insights into disease progression and treatment outcomes.
Conclusion
This study provides a comprehensive assessment of the global burden of lip and oral cavity cancer, revealing its increasing incidence, particularly among younger populations and women, as well as significant socioeconomic disparities. Although mortality rates have declined slightly, the disease burden remains disproportionately high in lower-income regions, emphasizing the need for improved prevention, early detection, and equitable healthcare access. Addressing these challenges requires a multidisciplinary approach that integrates pharmacotherapy, public health interventions, and healthcare policy reforms, to reduce disparities and improve patient outcomes.
References
-
Zheng CM, Ge MH, Zhang SS, et al. Oral cavity cancer incidence and mortality in China, 2010. J Cancer Res Ther. 2015;11(Suppl 2):C149–54. https://doi.org/10.4103/0973-1482.168176.
-
Kumar M, Nanavati R, Modi TG, et al. Oral cancer: etiology and risk factors: a review. J Cancer Res Ther. 2016;12(2):458–63. https://doi.org/10.4103/0973-1482.186696.
-
Dzebo S, Mahmutovic J, Erkocevic H. Quality of life of patients with oral cavity cancer. Mater Sociomed. 2017;29(1):30–4. https://doi.org/10.5455/msm.2017.29.30-34.
-
Zhang P, Lv D, Zhao J, et al. Evaluation of pharmacists’ interventions on drug-related problems and drug costs in patients with cancer pain. Int J Clin Pharm. 2021;43(5):1274–82. https://doi.org/10.1007/s11096-021-01247-w.
-
Shrestha S, Blebil AQ, Teoh SL, et al. Clinical pharmacists’ intervention on pain management in cancer patients (PharmaCAP trial): study protocol for a randomized controlled trial. J Pharm Policy Pract. 2023;16(1):14. https://doi.org/10.1186/s40545-022-00505-0.
-
Zhang C, Xiao J, Yu Z, et al. Cancer pain management and the roles of pharmacists in China. Int J Clin Pharm. 2021;43(2):383–5. https://doi.org/10.1007/s11096-021-01230-5.
-
Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–49. https://doi.org/10.3322/caac.21660.
-
Ferlay J, Colombet M, Soerjomataram I, et al. Cancer incidence and mortality patterns in Europe: estimates for 40 countries and 25 major cancers in 2018. Eur J Cancer. 2018;103:356–87. https://doi.org/10.1016/j.ejca.2018.07.005.
-
Blot WJ, McLaughlin JK, Winn DM, et al. Smoking and drinking in relation to oral and pharyngeal cancer. Cancer Res. 1988;48(11):3282–7.
-
D’Souza S, Addepalli V. Preventive measures in oral cancer: an overview. Biomed Pharmacother. 2018;107:72–80. https://doi.org/10.1016/j.biopha.2018.07.114.
-
Hübbers CU, Akgül B. HPV and cancer of the oral cavity. Virulence. 2015;6(3):244–8. https://doi.org/10.1080/21505594.2014.999570.
-
Miranda-Filho A, Bray F. Global patterns and trends in cancers of the lip, tongue and mouth. Oral Oncol. 2020;102:104551. https://doi.org/10.1016/j.oraloncology.2019.104551.
-
Cunha ARD, Compton K, Xu R, et al. The global, regional, and national burden of adult lip, oral, and pharyngeal cancer in 204 countries and territories: a systematic analysis for the global burden of disease study 2019. JAMA Oncol. 2023;9(10):1401–16. https://doi.org/10.1001/jamaoncol.2023.2960.
-
Du M, Nair R, Jamieson L, et al. Incidence trends of lip, oral cavity, and pharyngeal cancers: global burden of disease 1990–2017. J Dent Res. 2020;99(2):143–51. https://doi.org/10.1177/0022034519894963.
-
Kassebaum NJ, Smith AGC, Bernabé E, et al. Global, regional, and national prevalence, incidence, and disability-adjusted life years for oral conditions for 195 countries, 1990–2015: a systematic analysis for the global burden of diseases, injuries, and risk factors. J Dent Res. 2017;96(4):380–7. https://doi.org/10.1177/0022034517693566.
-
Ren ZH, Hu CY, He HR, et al. Global and regional burdens of oral cancer from 1990 to 2017: results from the global burden of disease study. Cancer Commun (Lond). 2020;40(2–3):81–92. https://doi.org/10.1002/cac2.12009.
-
Sun R, Dou W, Liu W, et al. Global, regional, and national burden of oral cancer and its attributable risk factors from 1990 to 2019. Cancer Med. 2023;12(12):13811–20. https://doi.org/10.1002/cam4.6025.
-
Zahiruddin QS, Jena D, Ballal S, et al. Burden of oral cancer and associated risk factors at national and state levels: a systematic analysis from the global burden of disease in India, 1990–2021. Oral Oncol. 2024;159:107063. https://doi.org/10.1016/j.oraloncology.2024.107063.
-
Yu Z, Ma X, Xiao H, et al. Disease burden and attributable risk factors of oral cancer in China from 1990 to 2021 and its prediction to 2031. Front Public Health. 2024;12:1419428. https://doi.org/10.3389/fpubh.2024.1419428.
-
GBD 2021 Diseases and Injuries Collaborators. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet. 2024;403(10440):2133–61. https://doi.org/10.1016/s0140-6736(24)00757-8.
-
GBD 2021 Risk Factors Collaborators. Global burden and strength of evidence for 88 risk factors in 204 countries and 811 subnational locations, 1990–2021: A systematic analysis for the Global Burden of Disease Study 2021. Lancet. 2021;403(10440):2162–203. https://doi.org/10.1016/s0140-6736(24)00933-4.
-
Board PDQPTE. Childhood Oral Cavity Cancer Treatment (PDQ®): Health Professional Version. PDQ Cancer Information Summaries. Bethesda (MD): National Cancer Institute (US); 2002.
-
Stevens GA, Alkema L, Black RE, et al. Guidelines for accurate and transparent health estimates reporting: the GATHER statement. Lancet. 2016;388(10062):e19–23. https://doi.org/10.1016/s0140-6736(16)30388-9.
-
Kim HJ, Fay MP, Feuer EJ, et al. Permutation tests for joinpoint regression with applications to cancer rates. Stat Med. 2000;19(3):335–51. https://doi.org/10.1002/(sici)1097-0258(20000215)19:3%3c335::aid-sim336%3e3.0.co;2-z.
-
Yao CZ, Zhang M, Zeng YK, et al. Analysis and prediction of thyroid cancer morbidity and mortality trends in China. Zhonghua Liu Xing Bing Xue Za Zhi. 2023;44(6):917–23. https://doi.org/10.3760/cma.j.cn112338-20221010-00869.
-
Das GP. A general method of decomposing a difference between two rates into several components. Demography. 1978;15(1):99–112.
-
Yang K, Yang X, Jin C, et al. Global burden of type 1 diabetes in adults aged 65 years and older, 1990–2019: population based study. BMJ. 2024;385:e078432. https://doi.org/10.1136/bmj-2023-078432.
-
World Health Organization. Handbook on health inequality monitoring with a special focus on low- and middle-income countries. (2013).
-
Ordunez P, Martinez R, Soliz P, et al. Rheumatic heart disease burden, trends, and inequalities in the Americas, 1990–2017: a population-based study. Lancet Glob Health. 2019;7(10):e1388–97. https://doi.org/10.1016/s2214-109x(19)30360-2.
-
Li Q, Ouyang X, Chen J, et al. A review on salivary proteomics for oral cancer screening. Curr Issues Mol Biol. 2020;37:47–56. https://doi.org/10.21775/cimb.037.047.
-
Lingen MW, Tampi MP, Urquhart O, et al. Adjuncts for the evaluation of potentially malignant disorders in the oral cavity: diagnostic test accuracy systematic review and meta-analysis-a report of the American Dental Association. J Am Dent Assoc. 2017;148(11):797-813.e52. https://doi.org/10.1016/j.adaj.2017.08.045.
-
Shamim MZM, Syed S, Shiblee M, et al. Automated detection of oral pre-cancerous tongue lesions using deep learning for early diagnosis of oral cavity cancer. Comput J. 2022;65(1):91–104. https://doi.org/10.1093/comjnl/bxaa136.
-
Warnakulasuriya S, Kerr AR. Oral cancer screening: past, present, and future. J Dent Res. 2021;100(12):1313–20. https://doi.org/10.1177/00220345211014795.
-
World Health Assembly. Seventy-fourth World Health Assembly: Geneva, 24 May-1 June 2021: resolutions and decisions, annexes. Geneva: World Health Organization; 2021.
-
World Health Organization. Global oral health status report: towards universal health coverage for oral health by 2030. Geneva: World Health Organization; 2022.
-
World Health Organization. Global strategy and action plan on oral health 2023–2030. Geneva: World Health Organization; 2024.
-
Kandalkar SS, Sharma M, Ahirrao B, et al. Assessment of prognostic indicators and survival-based impact of holistic approach in oral cancer patients: an observational study. Cureus. 2024;16(8):e67178. https://doi.org/10.7759/cureus.67178.
-
Rajput A, Gupta VK, Mishra G, et al. Comparative analysis of mouth self-examination awareness amongst tobacco users in urban and rural populations. Asian Pac J Cancer Prev. 2024;25(8):2805–12. https://doi.org/10.31557/apjcp.2024.25.8.2805.
-
Lei L, Zheng R, Peng K, et al. Incidence and mortality of oral and oropharyngeal cancer in China, 2015. Chin J Cancer Res. 2020;32(1):1–9. https://doi.org/10.21147/j.issn.1000-9604.2020.01.01.
-
Maomao C, He L, Dianqin S, et al. Current cancer burden in China: epidemiology, etiology, and prevention. Cancer Biol Med. 2022;19(8):1121–38. https://doi.org/10.20892/j.issn.2095-3941.2022.0231.
-
Sun D, Li H, Cao M, et al. Cancer burden in China: trends, risk factors and prevention. Cancer Biol Med. 2020;17(4):879–95. https://doi.org/10.20892/j.issn.2095-3941.2020.0387.
-
Qiu H, Cao S, Xu R. Cancer incidence, mortality, and burden in China: a time-trend analysis and comparison with the United States and United Kingdom based on the global epidemiological data released in 2020. Cancer Commun (Lond). 2021;41(10):1037–48. https://doi.org/10.1002/cac2.12197.
-
Deschler DG, Richmon JD, Khariwala SS, et al. The “new” head and neck cancer patient-young, nonsmoker, nondrinker, and HPV positive: evaluation. Otolaryngol Head Neck Surg. 2014;151(3):375–80. https://doi.org/10.1177/0194599814538605.
-
East KA, Reid JL, Rynard VL, et al. Trends and patterns of tobacco and nicotine product use among youth in Canada, England, and the United States from 2017 to 2019. J Adolesc Health. 2021;69(3):447–56. https://doi.org/10.1016/j.jadohealth.2021.02.011.
-
Lund L, Bast LS, Rubæk M, et al. Exploring factors associated with smokeless tobacco use among young people: a systematic scoping review. Drug Alcohol Depend. 2022;240:109627. https://doi.org/10.1016/j.drugalcdep.2022.109627.
-
Siddiqi K, Husain S, Vidyasagaran A, et al. Global burden of disease due to smokeless tobacco consumption in adults: an updated analysis of data from 127 countries. BMC Med. 2020;18(1):222. https://doi.org/10.1186/s12916-020-01677-9.
-
Guo SE, Huang TJ, Huang JC, et al. Alcohol, betel-nut and cigarette consumption are negatively associated with health promoting behaviors in Taiwan: a cross-sectional study. BMC Public Health. 2013;13:257. https://doi.org/10.1186/1471-2458-13-257.
-
Gupta B, Johnson NW, Kumar N. Global epidemiology of head and neck cancers: a continuing challenge. Oncology. 2016;91(1):13–23. https://doi.org/10.1159/000446117.
-
Lee YA, Li S, Chen Y, et al. Tobacco smoking, alcohol drinking, betel quid chewing, and the risk of head and neck cancer in an East Asian population. Head Neck. 2019;41(1):92–102. https://doi.org/10.1002/hed.25383.
-
Sarode G, Maniyar N, Sarode SC, et al. Epidemiologic aspects of oral cancer. Dis Mon. 2020;66(12):100988. https://doi.org/10.1016/j.disamonth.2020.100988.
-
Akyu Takei R, Tomihara K, Yamazaki M, et al. Protumor role of estrogen receptor expression in oral squamous cell carcinoma cells. Oral Surg Oral Med Oral Pathol Oral Radiol. 2021;132(5):549–65. https://doi.org/10.1016/j.oooo.2021.04.006.
-
Zhu S, Zhang F, Zhao G, et al. Trends in the global burden of oral cancer joint with attributable risk factors: Results from the global burden of disease study 2019. Oral Oncol. 2022;134:106189. https://doi.org/10.1016/j.oraloncology.2022.106189.
-
O’Reilly E, Frederick E, Palmer E. Models for pharmacist-delivered tobacco cessation services: a systematic review. J Am Pharm Assoc. 2019;59(5):742–52. https://doi.org/10.1016/j.japh.2019.05.022.
-
Madden M, Stewart D, Mills T, et al. Alcohol, the overlooked drug: clinical pharmacist perspectives on addressing alcohol in primary care. Addict Sci Clin Pract. 2023;18(1):22. https://doi.org/10.1186/s13722-023-00378-x.
Acknowledgements
We appreciate the GBD 2021 collaborators for their excellent work and selfless sharing.
Funding
This study was funded by the Natural Science Foundation of Hunan Province (No. 2024JJ9532), the Natural Science Foundation of Changsha City (No. kq2403178), Scientific Research Project of the Hunan Health Commission (No. D202313048136), the Chinese Medicine Research Project of Hunan Province (No. B2023048), and Joint Fund of Universities and Colleges (No. 2024XYLH290).
Ethics declarations
Conflicts of interest
The authors declare no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary file1 (DOCX 2970 kb)
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
Reprints and permissions
About this article
Cite this article
Hu, M., Chen, H., Wang, R. et al. Global, regional, and national burden of lip and oral cavity cancer and its attributable risk factors from 1990 to 2021: an analysis of the Global Burden of Disease study 2021. Int J Clin Pharm (2025). https://doi.org/10.1007/s11096-025-01961-9
- Received
- Accepted
- Published
- DOI https://doi.org/10.1007/s11096-025-01961-9
Keywords
- Disability-adjusted life years
- Epidemiology
- Global Burden of Disease
- Health inequalities
- Incidence
- Mortality
- Mouth neoplasms
- Risk factors