Article Content
Introduction
In the early fifteenth century, the notoriously famed Italian artist Leonardo da Vinci attempted the first fire protection system, called the automated fire sprinkler system, and designed a landscape garden with splendid fountains of running water for cooling wine, sprinkler systems for refreshing guests during hot summers, and automatic musical instruments played by water mills [1]. In 1812, the first fire protection system was called the fire sprinkler system and was invented and installed in Theatre Royal, Drury Lane, in London by architect William Congreve [2]. The automatic fire sprinkler head was subsequently improved by Henry Parmalee in 1874 and later perfected by Frederick Grinnell in the 1890 s [2]. While originally used to protect commercial buildings, fire sprinkler systems are now found in almost every building.
Fire sprinklers have saved countless lives over the years and continue to do so to this day, using much less water on average than that used by a firefighter’s hose [3]. Historically, fire sprinklers have been used for factories or large commercial properties; currently, they are utilized much more widely, including being installed most recently on residential properties [2].
A fire protection system is composed of appropriate electrical devices, equipment and systems used to detect a fire, activate an alarm, and suppress a fire [4]. According to Spitzenberger et al. [4], fire protection systems can be active or passive.
Chris Hani Baragwanath Academic Hospital (CHBAH) uses both active and passive fire protection systems, mainly sprinkler systems, deluge systems, wet systems, fire suppression systems, emergency light systems, fire detection systems, and fire alarm systems. Passive fire protection (PFP) systems attempt to slow the spread of fires and limit damage to building structures by providing occupants with time to escape safely or contain fires via fire equipment such as fire extinguishers.
PFP systems use fire-resistant materials that can be applied to firewalls, fire doors, and floors of buildings to delay the spread of fire. Spitzenberger et al. [4] noted that active fire protection (AFP) systems require motion detection and response mechanisms to work automatically or manually. The system can prevent fires from spreading and can extinguish fires once they are detected but requires people to deactivate them [4].
Roach [5] noted that balanced fire protection comprises sprinklers, automatic fire detection, and fire resistance-rated construction. The purpose and importance of fire protection systems are to detect fires, alert occupants to evacuate safely, extinguish fires, save lives, save property, and preserve business continuity depending on how a building is used and occupied [6].
The South African National Standard (SANS) 10,400-A [7] states that the level of fire protection that is required should be in line with the type of occupancy, use of space, and size and height of the building. Components such as gauges, valves, fire hydrants, and fire pumps are inspected visually on a weekly and monthly basis [8].
A disaster is an unforeseen and devastating event that significantly alters the functioning of a society or civilisation, resulting in human, material, and environmental losses greater than what it can manage on its resources [9]. There is no dispute that fires can break out at any time or anywhere without warning. When a fire breaks out, it can cause harm to people and severe property damage [10].
CHBAH is known as ‘Bara’ and is the largest public hospital in Africa and the third largest in the world [3]. It is situated at 26 Chris Hani Road and was built in 1942 in Diepkloof, a large zone of Soweto Township in southwest Johannesburg in Gauteng Province [11]. It is defined as an institution that provides medical, surgical, and nursing care for sick or injured people and operates on a 24-h basis [12]. CHBAH services an average of approximately 2,500 people per day over a 24-h operational time. This made the hospital one of the largest hospitals in the world in 1997 according to the Guinness Book of Records [13].
Torero [14] stated that the purpose of building classification is to determine the fire risk of a building, how to protect its occupants, and how to plan evacuation.
Hospitals use highly flammable substances and accommodate bedridden patients, elderly people, and sick people who cannot react immediately to an alarm when there is a fire emergency [15, 16].
Between 2011 and 2021, several hospitals in South Africa experienced fires, some of which were difficult to extinguish. These fires result in both life and property losses, amounting to millions of rands, and have negative socioeconomic impacts on the health and wellness of victims [17]. On 20 June 2021, CHBAH reported a fire in one of the back offices of the laundry area [18]. The office included a small laundry that was partially burnt. No one was injured, but this posed a serious threat to the safety of the occupants [19].
Literature review
The following literature review focuses on addressing Research Question 1, Research Question 2, Research Question 3, and Research Question 4. The study was designed to achieve the following objectives:
- 1.To assess the state of the fire protection system
- 2.To advise on the best maintenance practice
- 3.To adopt the best practice regarding safety at the hospital
- 4.To understand the perceptions of hospital staff on the fire protection system
- Research Question 1: Current State of Fire Protection Systems: What is the current condition of fire protection systems in hospitals, and how does it impact staff safety.
Several fires that occurred at CHBAH, fire extinguishers that were used to extinguish the fires or, when used during training, were not being reserviced and mounted back on the wall with signage for it and were missing in other areas. If CHBAHs experience a fire incident, they will be unable to suppress or extinguish small fires in their early stages, which will lead to uncontrolled fires that will spread and cause loss of life and property.
At CHBAH, the installed fire horns did not meet any South African standard codes in terms of warning occupancies and had no proof of being tested for approval as a warning system to be used at the hospital. Fire horns were not designed to replace the approved warning system per the South African National Standard (SANS) codes; instead, they serve as a backup system. They were not visual for occupants who cannot hear and see which impact on evacuation when there was a fire incident.
- Research Question 2: Best Practices for Fire Protection Maintenance: How does regular maintenance of fire protection systems in hospitals affect fire safety compliance and risk reduction.
In accordance with the South African National Standard, SANS 1475–2 [20], fire hydrants should undergo regular inspection and testing at least once a year, unlike at CHBAH. During inspection, the water pressure of underground and above-ground fire hydrants is crucial. It should be maintained at a minimum of 300 kPa (kilopascal). Adequate water pressure ensures that firefighters can access water effectively when needed.
According to the City of Johannesburg [21] guidelines, it is important to record the results of inspection and testing. This documentation helps in tracking the maintenance history of each hydrant, ensures accountability and can help ensure that fire hydrants are reliable during emergencies.
- Research Question 3: International Hospital Safety Practices: What are the best international practices for hospital safety, and how do they compare across different healthcare systems.
The fire protection systems of the CHBAH should always comply with safety regulations that were approved at the time it was built. If there are any building alterations, demolitions, or renovations, they must be in line with the current City of Johannesburg Emergency Management Services bylaws, South African National Standard: 10,040-Part -A, Part -T, Part -S and Part -W, National Building Regulations (Act 103 of 1977), Occupational Health and Safety Act, 85 of 1993 (SA, 1993), and other regulations that are commonly used in South Africa.
Furthermore, the National Building Regulations and Building Standard (Act 103 of 1977) is satisfied if only a building is constructed and equipped with everything required by the SANS 10400-T [15, 16]. In addition, local authorities must also be satisfied with the design and plan of the building before construction can begin.
According to the National Fire Protection Association [22], fire protection requirements and guidelines must be adopted from standard codes that are relevant to hospitals and healthcare facilities for compliance. The goal of this code is a fire risk assessment to provide an environment for occupants that is reasonably safe from fire and similar emergencies. It is also the most comprehensive code addressing the minimum building design, construction, operation, and maintenance requirements necessary to protect building occupants from danger caused by fire, smoke, toxic fumes, and similar emergencies in both new and existing buildings [22].
- Research Question 4: Hospital Staff Perceptions of Fire Safety: What are hospital staff perceptions of fire protection systems, and how do these perceptions influence safety culture and preparedness.
The literature indicates that many healthcare institutions struggle with consistent fire safety practices, often leading to insufficient preparedness and response during fire emergencies. Hospital staff often have varying levels of knowledge and understanding of fire protection systems in their facilities at CHBAH.
According to a survey conducted by Harris [23], many healthcare workers expressed uncertainty about their role during a fire emergency, primarily due to inadequate training and a lack of regular fire drills. Most hospital staff advocated for improved training and education regarding fire protection systems. However, respondents reported concerns about maintenance and functionality in most of the CHBAH buildings. Staff indicated that frequent testing and maintenance of these systems were necessary to ensure reliability in emergencies, emphasizing that operational systems are only as effective as their upkeep.
Jones et al. [24] reported that frequent training sessions significantly improved staff confidence and competence in using fire extinguishers and executing evacuation procedures. A study by Smith and Brown [25] reported that sporadic training resulted in a lack of familiarity with emergency protocols, which can exacerbate risks during a fire incident.
The perceptions of hospital staff regarding fire protection systems are shaped by their awareness, confidence, perceived effectiveness, and barriers encountered in the use of the systems. The literature emphasizes the need for comprehensive fire risk assessments and tailored fire safety measures that address the unique challenges of facilities.
History of Chris Hani Baragwanath Academic Hospital fires
According to Lesia [18], ten fire incidents in various sections of the hospital were reported from 2018 to 2022 to the management to be documented and investigated. However, not all fires were reported to the City of Johannesburg Emergency Management Services (local fire department) for their service to be rendered, as some of those fires were extinguished before their arrival and contained using some of the fire protection systems that exist at CHBAH (like fire extinguishers and hose reels).
These fires happened during all seasons of the year, which were in autumn, winter, spring, and summer (see Table 1) which shows the data documented and reported about the fire incidents at CHBAH).
Comparison of variables using Pearson chi-square
Cross-tabulation, also known as contingency table analysis, is a statistical technique to help understand the relationship between two or more variables. The analysis was conducted using the following demographics about participants: which category of workgroup do they belong to at their workplace, and how many years of service have they had at the hospital? It allows an exploration of patterns, dependencies, and associations in the dataset. Comparing the variable of Part A: Demographics, with variables from Part B: Basic knowledge of fire safety fire equipment, Part C: Fire equipment, and Part D: Application. Pearson’s chi-square was used to measure a significant relationship between two categorical variables, and a significant relationship was observed when the p-value was less than 0.05.
Part A: Demographics versus Part B: Knowledge of fire safety
| Code | Label |
|---|---|
| N | Represent the number of participants |
| % | Represent percentage |
| Vs | Versus |
| Accepted | This means there is a significant relationship between the variables |
| Rejected | This means there is no significant relationship between the variables |
Table 2 is a frequency table representing the workgroup of participants who could define a fire: specialists, doctors, or nurses (n = 107) at a percentage value of 72.8% answered correctly that fire is a chemical reaction that releases light and heat, general workers, or staff (n = 52) at a percentage value of 47.3%, top management (n = 4) at a percentage value of 36.7%. Therefore, there was a relationship between which work category the participants belonged to versus the definition of a fire, with a p-value of Pr = 0.001 (Accepted), which was less than the significant level of a p-value of Pr = 0.05.
Table 3 is a frequency table representing the workgroup of participants who knew the elements of a fire: specialists, doctors, or nurses (n = 108) at a percentage value of 73.5% answered correctly saying heat, oxygen, and fuel are elements of fire, top management (n = 8) at a percentage value of 72.7%, general workers or staff (n = 56) at a percentage value of 50.9%. The frequency table shows that there was a relationship between the participants’work group and their knowledge of the elements of fire. The table indicates that specialists, doctors, or nurses had a higher percentage of correct answers compared to top management and general workers or staff with a p-value of Pr = 0.009 (Accepted), which was less than the significant level with a p-value of Pr = 0.05.
Table 4 is a frequency table representing the workgroup of participants who could identify what a fire extinguisher was not: top management (n = 10) at a percentage value of 90.9% answered correctly, specialist, doctor, or nurse (n = 97) at a percentage value of 66.0%, general workers or staff (n = 50) at a percentage value of 45.5%. Therefore, there was a relationship between the workgroup category and knowledge about fire extinguishers with a p-value of Pr = 0.000 (Accepted), which was less than the significant level with a p-value of Pr = 0.05.
Table 5 is a frequency table representing the number of years a participant has worked at the hospital correlated to whether they know what is not a fire extinguisher: 0 to 5 years (n = 72) at a percentage value of 69.2%, 6 to 10 years (n = 33) at a percentage value of 58.9%, 11 to 20 years (n = 32) at a percentage value of 50.0%, over 21 years (n = 20) at a percentage value of 45.5%. The data shows that there was a relationship between years of service at the hospital and the ability to select what is not a fire extinguisher. The frequency table suggests that as the number of years of service increases, the percentage of individuals who answered correctly decreases with a p-value of Pr = 0.006 (Accepted), which was less than the significant level with a p-value of Pr = 0.05.
Table 6 is a frequency table representing the years of service and the ability to identify the purpose of fire alarms and smoke detectors: 6 to 10 years (n = 55) at a percentage value of 98.2%, 0 to 5 years (n = 101) at a percentage value of 97.1%, over 21 years (n = 38) at a percentage value of 86.4%, 11 to 20 years (n = 55) at a percentage value of 85.9%. Therefore, there was a relationship between how many years of service at the hospital versus what is the purpose of a fire alarm and smoke detector with a p-value of Pr = 0.003 (Accepted), which was less than the significant level with a p-value of Pr = 0.05. This indicates that the relationship between the two variables was statistically significant.
Part A: Demographics versus Part C: Fire equipment
Table 7 is a frequency table representing the workgroup of participants and how they identify fire equipment identifying fire equipment by its colour codes, signage, and their purpose: specialists, doctors, or nurses (n = 134) at a percentage value of 91.2% answered correctly, top management (n = 10) at a percentage value of 90.9%, general workers or staff (n = 79) at a percentage value of 71.8%. Therefore, there was a statistically significant relationship between the category of the workgroup to which the participants belong and how they identified fire equipment with a p-value of Pr = 0.002 (Accepted), which was less than the significant level with a p-value of Pr = 0.05.
Table 8 is a frequency table representing the participants’years of service who answered yes to having fire protection system service history records: 11 to 20 years (n = 25) at a percentage value of 39.1%, 6 to 10 years (n = 21) at a percentage value of 37.5%, over 21 years (n = 14) at a percentage value of 31.8%, 0 to 5 years (n = 19) at a percentage value of 18.3% answered yes. Therefore, there was a significant relationship between the number of years of service at the hospital and the presence of records for fire protection systems, with a p-value of Pr = 0.008 (Accepted), which was less than the significant level with a p-value of Pr = 0.05.
Part A: Demographics versus Part D: Application
Table 9 is a frequency table representing the workgroup category of participants who knew that trained fire marshal safety officers coordinate emergencies at the hospital: top management (n = 9) at a percentage value of 81.8%, general workers or staff (n = 67) at a percentage value of 60.9%, specialists, doctors, or nurses (n = 56) at a percentage value of 38.1%. The analysis concludes that there was a relationship between the workgroup category and knowing who coordinates emergencies during an emergency in the hospital with a p-value of Pr = 0.000 (Accepted), which was less than the significant level with a p-value of Pr = 0.05.
Table 10 is a frequency table representing participants’ years of service and their knowledge that the hospital has trained fire marshals and safety officers: over 21 years (n = 21) at a percentage value of 47.7% answered yes, 6 to 10 years (n = 23) at a percentage value of 41.1%, 11 to 20 years (n = 25) at a percentage value of 39.1%, 0 to 5 years (n = 26) at a percentage value of 25.0%. Therefore, the frequency table shows the percentage values of various work groups coordinating emergencies at a hospital, and the statistical analysis suggested a significant relationship between the work category and emergency coordination, with a p-value of Pr = 0.006 (Accepted), which was less than the significant level with a p-value of Pr = 0.05.
Summary
The analysis of questionnaires distributed at CHBAH focused on the state of fire protection systems. Participants were asked to answer the questionnaires based on their knowledge, training, experience, and awareness of the existence of fire protection systems at the hospital. The findings were discussed in Parts A, B, C, and D. Using the Pearson chi-square statistical test, of the 27 measured questions, only nine questions showed a significant relationship. This means that for these nine questions, there was evidence of a relationship between the measured variables. The significance level used was Pr = 0.05, which means that if the p-value associated with a question was less than 0.05, it was considered statistically significant.
Materials and methods
A mixed-methods approach with cross-sectional analysis was employed. The study included hospital community members, with the exclusion of patients, visitors, and student nurses. Obtaining informed consent from critically ill or vulnerable patients at CHBAH was challenging, as their condition may have hindered their ability to fully understand the study’s risks and benefits, raising ethical concerns. Strict privacy laws like the Protection of Personal Information Act 4 of 2013 (“POPIA”) in South Africa limited patient data use, while research activities risked disrupting hospital care, requiring a balance between study goals and patient well-being. Institutional reviews often rejected high-risk studies, and since patients and visitors were less representative or available, the research focused more on CHBAH staff for reliable data. The data were collected through self-administered structured questionnaires, building observations using checklist, and face-to-face in-depth interviews for three months in 2022. Simple random sampling and sequential convenient nonprobability sampling methods were used to select the buildings and study participants.
The Cochran’s Formula was used in the study to determine an appropriate sample size for selecting 130 buildings at CHBAH. Therefore, Cochran’s Formula was used to calculate a statistically valid sample size that ensured a representative and reliable analysis while maintaining an acceptable margin of error. The sample size was determined with the Z statistic (Z2 = 1.96) at a 95% confidence interval (95% CI), an expected response distribution (p) of 20%, and a 5% margin of error using the Cochran formula [26].
where:
- n0 = Required sample size
- Z = Z-score (based on confidence level, e.g., 1.96 for 95% confidence)
- p = Estimated proportion of the population with the characteristic of interest (typically 0.5 if unknown)
- e = Margin of error (precision level, e.g., 0.05 for 5%)
Therefore, for finite populations, the sample size was adjusted using Cochran formula [26] and where N was the total population size.
Sequential convenient nonprobability sampling was used to select two hundred eighty research participants. Only two hundred and sixty-eight questionnaires were returned from the two hundred and eighty questionnaires distributed. The study participants were of different genders according to the questionnaires, and interviews and informed consent were obtained from all those involved in the study (including the interviewees). For the interviews, six participants (n = 6) volunteered out of the 13 top management staff, and they were selected. For observation, a total of 130 buildings were inspected via a checklist.
Data analysis
Quantitative analysis
For observation and questionnaire analysis, data were captured via Microsoft (MS) Excel and converted into the Statistical Package for Social Sciences (SPSS) for quantitative analysis. The descriptive analysis results are presented in the form of frequency tables and charts.
Qualitative analysis
The data from the interviews were analysed via thematic analysis (see Fig. 1). The process involved transcribing all the recorded audio interviews and identifying codes, which were further grouped into common themes and subthemes [27] (see Fig. 9).
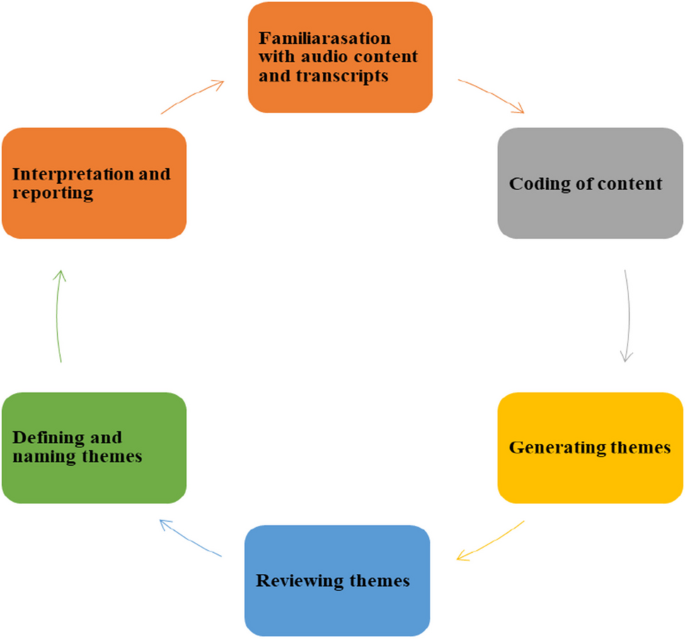
The thematic analysis processes
Quantitative and qualitative results
Quantitative results
Questionnaires
The questionnaires included 27 questions and consisted of four parts: Part A: personal information; Part B: basic knowledge of fire safety; Part C: fire equipment; and Part D: application (the ability of participants to use knowledge and fire equipment during an emergency).
For gender
The demographic variables (including gender: male, female, and other) were collected because, historically, hospitals had more women than men working there. The study determined which sex was most represented at the hospital. Figure 2 shows the participants’ personal information according to sex. Most of the respondents were female (n = 159), accounting for 59.0%, and there were fewer male participants (n = 109) than female participants, accounting for 41.0%. This means that there are still more women at CHBAH than men.
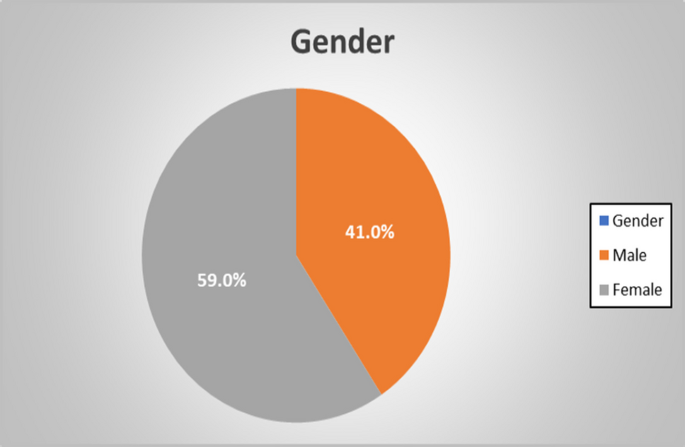
Participants’ personal information by sex
For years of service
The number of years of service was asked to provide a history of the individual regarding experiences at the hospital. The length of employment is an indicator of how often an employee was trained during employment. Figure 3 shows the participants’ personal information under years of service at the hospital. The highest number of participants in this category was 0–5 years (n = 104) at a percentage value of 39.0%, 11–20 years (n = 64) at a percentage value of 24.0%, and 6–10 years (n = 56) at a percentage value of 21.0%, followed by those older than 21 years (n = 44) at a percentage value of 16.0% as the lowest category.
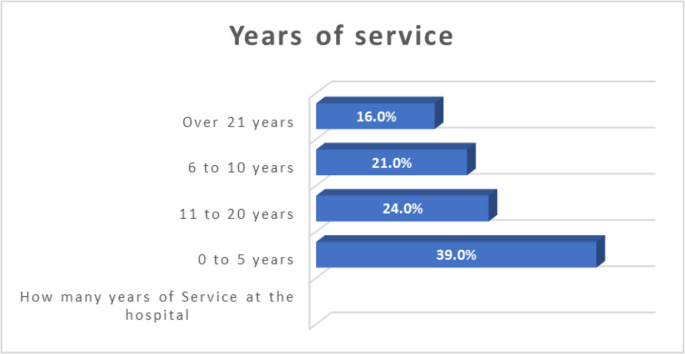
Participants’ personal information under years of service at the hospital
The notification system or device used at the hospital
The participants were requested to identify the notification system or device that was used at the hospital to determine which device they knew at the hospital. Figure 4 represents the participants (n = 113) at a percentage value of 42.0% who answered the fire horn as a notification or device used at the hospital when there was a fire; participants (n = 78) at a percentage value of 29.0% answered siren; participants (n = 35) at a percentage value of 13.0% answered that none of the devices were used at the hospital when there was a fire; participants (n = 20) at a percentage value of 8.0% answered a cell phone; participants (n = 14) at a percentage value of 5.0% answered manual pull station; and participants (n = 8) at a percentage value of 3.0% answered a PA system.
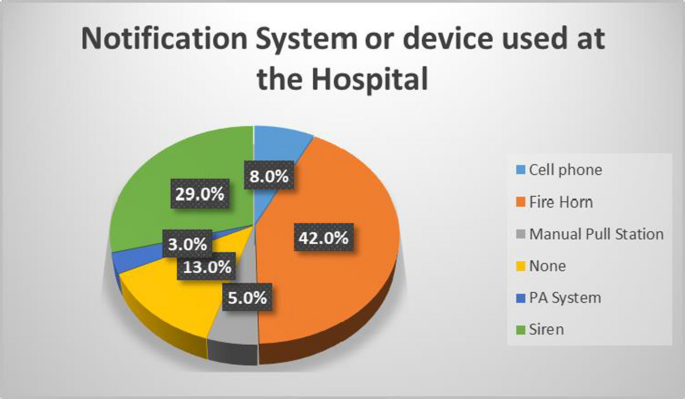
shows the notification system or device used at the hospital
Quantitative results
Observations
This section addresses the quantitative results of visual observations from a simple random sample selection of 130 buildings from 407 buildings identified and selected at CHBAH via a checklist with sections. Eight qualified senior inspectors and inspectors (safety officers) from the City of Johannesburg Emergency Management Services (COJEMS) under the Pro-Active Services section assisted in conducting visual observations of the CHBAH buildings. The following building codes were created on the checklist: 0 – Noncompliant, 1 – Partially compliant, 2 – Compliant, and 3 – Fully compliant (see Table 11).
Under section A11 (evacuation plan)
The requirements of section A11 include evacuation plan approval by the local fire department, which is available and displayed on the wall. Figure 5 shows the results for the A11 evacuation plan. Of a simple random sample of 130 buildings observed, 12 buildings did not require an evacuation plan, while 113 buildings did not have stamped A11 evacuation plans at a percentage value of 96.0% (noncompliant), and five buildings had stamped A11 evacuation plans available onsite at a percentage value of 4.0% (compliant).
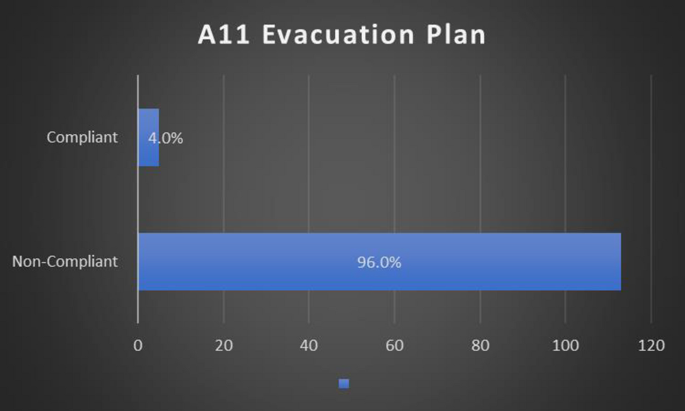
Results for A11 in the evacuation plan
Under section A13 (assembly points)
The section A13 requirements include assembly points on the evacuation plan with signage outside the hospital building. Figure 6 shows the results for the A13 assembly points. Of a simple random sample of 130 buildings observed, 12 buildings did not require assembly points to be installed, 109 buildings did not have A13 assembly points at a percentage value of 92.0% (noncompliant), and nine buildings had A13 assembly points at a percentage value of 8.0% (compliant).
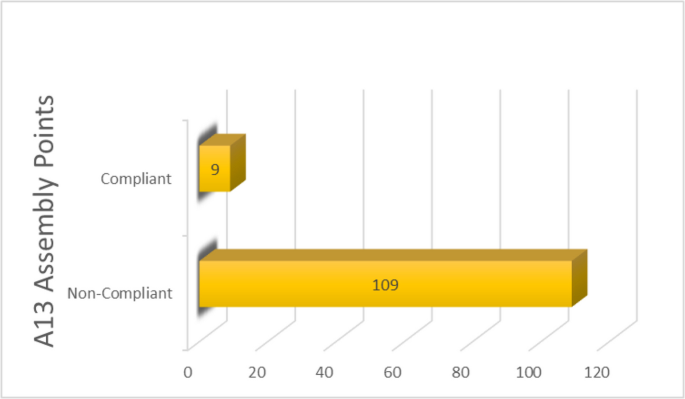
Results for A13 assembly points
Under section C2 (fire alarm)
The section C2 requirements include fire alarms available in all the required areas. Figure 7 shows the results for the C2 fire alarm. Of a simple random sample of 130 buildings observed, 16 buildings did not require fire alarms to be installed, 102 buildings observed did not have C2 fire alarms at a percentage value of 89.5% (noncompliant), and 12 buildings observed had C2 fire alarms at a percentage value of 10.5% (compliant).
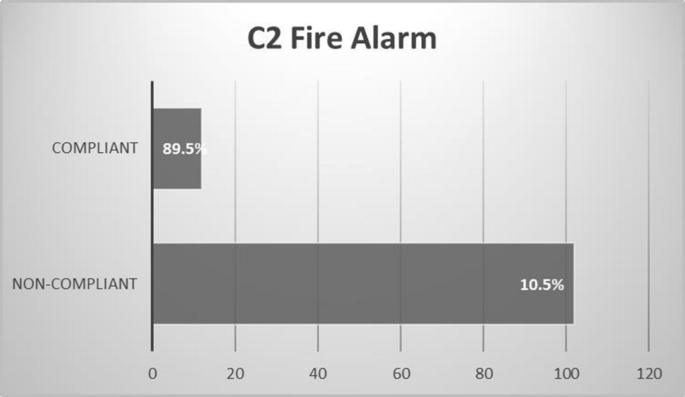
Results for the C2 Fire Alarm
Under section H2 (fire extinguisher location)
The requirements of section H2 include that fire extinguishers are mounted on walls without obstructions. Figure 8 shows the results for the H2 fire extinguisher location. Among a simple random sample of 130 buildings observed, one building did not require a fire extinguisher location, whereas 74 buildings observed did not have an H2 fire extinguisher location at a percentage value of 57.0% (noncompliant), and 55 buildings observed had an H2 fire extinguisher location at a percentage value of 43.0% (compliant).
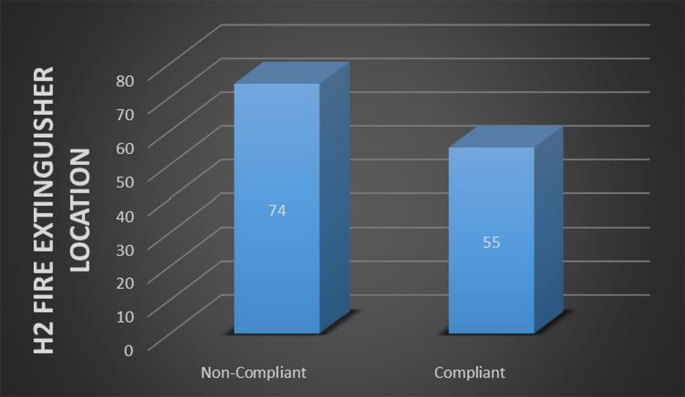
Results for H2 fire extinguisher location
Qualitative results
Interview
To ensure the anonymity of the respondents, the following pseudonyms were used: respondent 1, respondent 2, respondent 3, respondent 4, respondent 5, and respondent 6 (see Table 12).
The qualitative section presents the themes developed during face-to-face structured in-depth interviews with six permanent staff members (top management) of the CHBAH who volunteered to participate in the study in 2022. The following themes emerged during the data analysis: knowledge of fire safety protocols, fire safety certification and compliance, fire incident reporting and investigations, training and capacity building, routine inspections and maintenance, and stakeholder collaboration. Figure 9 shows the thematic analysis process and the resulting themes.
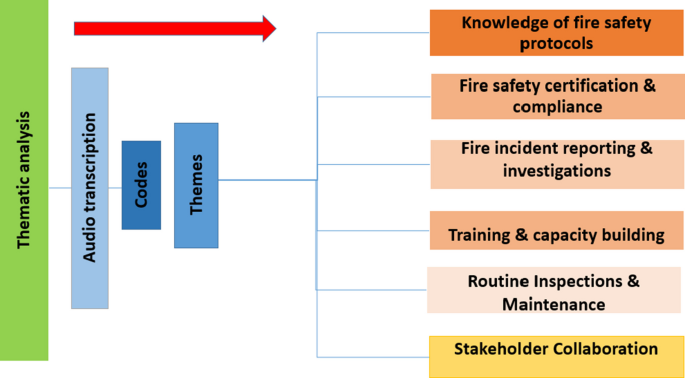
Thematic analysis process and resultant themes
Knowledge of fire safety protocols
Most of the respondents were not familiar with the fire safety protocols that are important for individuals in hospitals or hospital staff members. Furthermore, no training was provided for any of the staff, including for COVID-19 contract nurses employed during the COVID-19 pandemic (2019–2022).
Fire safety certification and compliance
The respondents had various responses to this question. Some indicated the presence of a disaster plan, which included fire emergencies. An emergency plan was created by a retired professor, which indicated that it was not reviewed, whereas others reported that the hospital had no fire emergency plan in place, only standard operating procedures. Some respondents stated that emergency plans in which there were either not readable or hand drawn.
Fire incident reporting and investigations
The respondents indicated that all the fire incidents were reported and that the staff were cooperative. The reports are deduced to be true reflections on the fire incidents that occurred at the hospital on the basis of the interview questions. Evidence and records of fire incidents at CHBAH were reported from 2018–2022, and the management of these incidents was documented and investigated. Importantly, however, the reporting of fire incidents was a common component that was frequently mentioned by all the respondents.
Training and capacity building
According to the interviews, training on fire safety was sporadic and deficient. Some respondents indicated that they had not had a fire drill in two to four years, as previously stated. A total of 33.3% of the staff members reported a lack of training and capacity building because fire drills were not conducted, 33.3% indicated that, owing to budget constraints, fire drills were rarely conducted, 16.7% mentioned that drills were conducted annually, and 16.7% reported that fire drills were only conducted at their department, not the entire CHBAH.
Routine inspection and maintenance
The respondents provided different answers, revealing various stakeholders who may or may not be responsible for maintenance. However, it was unclear what the working relational dynamics were and who was responsible for which action concerning maintenance. Some respondents indicated the facility management unit (FMU) or the Department of Infrastructure and Development (DID). These responses suggest that routine inspections have not been performed for all 407 buildings in the hospital but have been performed for only some. This is also an indication of a lax approach to the maintenance and inspection of fire equipment, especially when in-house training is performed at the laundry.
Stakeholder collaboration
The interview results indicate significant issues with stakeholder engagement, communication, and collaboration regarding fire safety. The respondents highlighted concerns such as inadequate service of fire equipment, negligence among staff, lack of adherence to management directives concerning heating sources, unaddressed requests for alternative heating by the DID, and the need for improved awareness and training in fire safety protocols. There appears to be a clear demand for better collaboration between units responsible for occupational health and safety (OHS) and unit managers to enhance overall fire safety measures.
Discussion
The study conducted at CHBAH revealed significant concerns regarding fire safety preparedness, equipment compliance, and staff awareness. The research, based on questionnaires, observations, and interviews, highlighted that the length of employment influenced employees’exposure to training and emergency experiences, with newer staff (0–5 years) forming the largest group (39%). However, a substantial portion of participants lacked basic fire safety knowledge, with 62.7% unaware of fire classes, and 6.7% providing incorrect answers. This gap in knowledge underscores the need for continuous and updated fire safety training. Additionally, the use of non-compliant fire horns as the primary warning system (42%) and the lack of awareness about trained fire marshals (48.5% unsure) further indicate deficiencies in emergency preparedness. The study also found inconsistencies in the hospital’s emergency plan, with contradictory responses from staff, suggesting poor communication and coordination.
Observations revealed alarming levels of non-compliance with fire safety standards across CHBAH buildings. Only 5% of buildings had proof of fire clearance, and 96% lacked approved evacuation plans. Key safety equipment, such as fire alarms (89.5% non-compliant), smoke detectors (94% non-compliant), and fire doors (54% non-compliant), were either missing, malfunctioning, or improperly maintained. The absence of kitchen fire suppression systems in all buildings posed a significant risk, given the potential for rapid fire spread. Furthermore, inadequate signage, obstructed fire extinguishers, and non-functional manual call points further compromised safety. These findings highlight critical gaps in fire safety infrastructure, training, and compliance, necessitating urgent intervention to ensure the safety of patients, staff, and visitors. Regular drills, updated training, and adherence to national safety standards are essential to address these deficiencies and improve emergency preparedness at CHBAH.
Conclusions
This conclusion, presents questionnaires, interviews, and observations regarding the fire protection system at CHBAH and explores the implications of these findings, focusing on the adequacy of the fire protection system, staff knowledge, and emergency preparedness. The study revealed significant non-compliance with fire safety standards, including inadequate staff training, outdated equipment, and poor maintenance practices. These issues pose serious risks to the safety of CHBAH occupants and the continuity of operations during fire emergencies. This conclusion emphasizes the urgent need for corrective actions, including improved training, regular drills, and adherence to safety regulations, to enhance fire safety at CHBAH.
The research highlighted several critical areas of concern, such as the lack of awareness among staff regarding fire safety protocols, inconsistent evacuation drills, and the absence of a clearly communicated emergency plan. Additionally, the study found that many buildings at CHBAH were non-compliant with fire safety standards, lacking essential features like functional fire alarm systems, proper evacuation plans, and adequate fire suppression systems. Staff perceptions of the fire protection system varied, with some expressing confidence in the system while others raised concerns about equipment malfunctions and insufficient training. The study concludes by recommending further research and immediate interventions to address these deficiencies, ensuring a safer environment for patients, students, and visitors. The findings underscore the importance of fostering a culture of safety and accountability within the hospital to mitigate fire-related risks effectively.
Potential barriers to implement the recommendations and how to overcome the challenges
Implementing the recommendations for improving fire safety at CHBAH may face several barriers, including financial constraints, bureaucratic delays, and resistance to change. The CHBAH may struggle to secure sufficient funding for infrastructure upgrades, such as building a mini-fire station, installing advanced fire detection systems, or conducting regular maintenance. Additionally, coordinating efforts among multiple departments (e.g., DID, FMU, OHS) and external stakeholders (e.g., COJEMS, contractors) could lead to administrative inefficiencies and delays. Resistance from staff, particularly regarding changes to established routines or the introduction of new protocols, may also hinder progress. Furthermore, the complexity of retrofitting existing buildings to meet fire safety standards while maintaining hospital operations poses significant logistical challenges.
To overcome these barriers, a multi-faceted approach is necessary. First, securing dedicated funding through government allocations, grants, or partnerships with private entities can address financial limitations. Streamlining communication and decision-making processes among departments and stakeholders through regular meetings and clear accountability structures can reduce bureaucratic delays. Engaging staff through comprehensive training, awareness campaigns, and involving them in the planning process can foster buy-in and reduce resistance. Prioritizing phased implementation of recommendations, starting with high-risk areas, can help manage logistical challenges while minimizing disruption to hospital operations. Finally, leveraging technology, such as integrated building management systems, can enhance efficiency and ensure compliance with fire safety standards. By addressing these barriers proactively, CHBAH can create a safer environment for its community.