Article Content
Abstract
This exploratory single-session case study aimed to gain insight into the added value of measuring heart rate variability in enhancing the understanding of the emotions and meanings involved in the dialog between a client with an anxiety disorder and a psychotherapist. Heart rate variability was measured in both clients and psychotherapists, and the root mean square of successive differences in heartbeats was used as a proxy to parasympathetic nervous system activation. Associations between the themes of the dialog and the psychophysiological markers were examined. The study demonstrated that changes in heart rate variability exhibited logical associations with ongoing dialog themes. The study yielded insights into the client’s emotional state, particularly in instances where she expressed guilt- and shame-provoking emotions and thoughts, and when the psychotherapist sought to provide empathy and validation that the client was unable to receive or accept. The first finding suggests that parasympathetic activation may increase as repressed thoughts or emotions are verbalized. The latter finding supports the claim that sympathetic activation may be elevated in response to experiences that do not align with an individual’s identity narrative. Additionally, the psychophysiological data suggested that the client’s emotions were more intense than could be inferred from her voice or facial expressions. Notwithstanding the necessity to exercise caution when interpreting the findings based on a single psychotherapy session, the results suggest that psychophysiological indices have the potential to enhance understanding of client and psychotherapist processes during therapeutic interactions. Thus, further research using psychophysiological markers in clinical settings seems justified.
Explore related subjects
Discover the latest articles and news from researchers in related subjects, suggested using machine learning.
- Emotion Regulation
- Person-Centered Psychotherapy
- Physiological Psychology
- Psychodynamics
- Psychological Assessment
- Psychotherapy
Introduction
The relevance of emotions to an individual’s functioning and well-being has long been recognized, and emotions have been acknowledged as central to therapeutic change (Lane et al., 2022). Hence, several theories have emerged providing insights into the psychophysiological and cognitive processes related to the complexity of emotional processing and emotion regulation, many focusing on the role of the autonomic nervous system, like polyvagal theory (Porges, 2022) and the neurovisceral integration model (Smith et al., 2017). As most of the research on psychophysiological processes has been conducted in experimental settings, further research in clinical settings is needed to better understand whether measuring psychophysiology has added value to understanding clients’ experiences.
Psychophysiological research in the field of psychotherapy has mainly concerned either between-person associations (e.g., synchrony between the participant) or within-person associations (e.g., correlations between client experience and physiology; Deits-Lebehn et al., 2020). In this exploratory single-session case study, we focused on the individual physiology. We analyzed heart rate variability (HRV), that is, the variation in the time between successive heartbeats, from both the client and the therapist during one psychotherapy session and evaluated the relationships between changes in HRVs and the psychotherapy dialog.
Heart Rate Variability (HRV) as an Indicator of Physiological Arousal
Harth rate is influenced by both autonomic nervous systems and by changes in muscle tonus and respiratory sinus arrhythmia related to in- and out-breathing (Grossman & Taylor, 2007). An increase in heart rate is related to sympathetic activation, which corresponds to, for example, an increase in vigilance, active avoidance, and unpleasant affect. Conversely, a reduction in heart rate is associated with parasympathetic activation, which is linked to positive affect and cognitive processing. A more detailed examination of the sympathetic and parasympathetic components can be conducted by measuring HRV, which reflects the activation of both sympathetic and parasympathetic activation. In response to a threatening stimulus or an experience of anxiety or tension, the sympathetic system becomes more active, while the parasympathetic becomes less active. As a result, HRV is diminished (e.g., Gullett et al., 2023). In the opposite situation, when a person is at rest and does not experience a significant internal or external threat or stress, the parasympathetic system is more active in relation to sympathetic system.
HRV has been linked to emotional responses and emotion regulation (Balzarotti et al., 2017; see polyvagal theory: Porges, 2022), as it has been identified to reflect the ability to adjust arousal on a moment-by-moment basis (Pham et al., 2021). Those with high HRV appear to better adapt their response to situational demands, whereas those with low HRV show a failure to recognize safety signals and activation of a defensive system even in response to non-threatening stimuli (see neurovisceral integration model: Thayer & Brosschot, 2005). Accordingly, HRV has been suggested to reflect the individual’s experience of safety (Petrocchi & Cheli, 2019) or feeling understood (Deits-Lebehn et al., 2020), which can be considered key elements in psychotherapy.
The commonly used HRV index of time domain analysis is the root mean square of successive differences between heartbeats (root mean square of the successive R-R differences [RMSSD]), which quantifies the amount of variability in time between successive heartbeats (Shaffer & Ginsberg, 2017). In the present study, we used RMSSD, as it has been claimed that HRV frequency domain analyses should not be used as an index of vagal activity in tasks requiring verbal responses, as they may induce respiratory changes distorting the index (Thomas et al., 2019). RMSSD is statistically robust (Pham et al., 2021) and suited for short-term time windows (Shaffer & Ginsberg, 2017). Despite being sensitive to both sympathetic and parasympathetic activation, RMSSD is more influenced by the parasympathetic activity and has been used to estimate the vagally mediated fluctuations in heart rate (Pham et al., 2021). It can be interpreted as a proxy for parasympathetic activation (Laborde et al., 2017) and has been associated with diverse emotional experiences (e.g., anger; Wu et al., 2019; sadness Gullet et al., 2023; Sin et al., 2016). However, in addition to emotional processing, RMSSD also reflects, for example, cognitive processing, physical movement, and respiratory patterns. Therefore, simplistic interpretations should be avoided.
Measuring Autonomic Nervous System in Therapy Studies
Clinical research has shown that clients’ emotional expression during therapy interactions is associated with autonomic arousal and is influenced by therapist behavior (Del Piccolo & Finset, 2018). Couple therapy studies using electrodermal activity to analyze of the autonomic nervous systems changes in relation to the therapeutic dialog have indicated greater emotional arousal when an identity-threatening accusation emerged in the discussion (Päivinen et al., 2016) and after the therapists’ intervention (Laitila et al., 2019). Likewise, Kykyri et al. (2024) found that synchrony in couples’ electrodermal activities was associated with nonverbal emotional expression, emotional valence, and topics of conversation.
In accordance with the idea of autonomic reaction reflecting, among other things, the experience of safety (e.g., Deits-Lebehn et al., 2020; Porges, 2022), measurements done during therapy sessions have shown relation to the therapeutic collaborative relationship (Blanck et al., 2019). In a study with patient–therapist dyads, Marci et al. (2007) found a significant positive correlation between skin conductance concordance and patient ratings of perceived empathy. By integrating verbal, nonverbal and physiological data, Mylona et al. (2023) showed how the repair of an alliance rupture entailed increased relatedness between the client and the therapist and simultaneous physiological synchronization. Activity of the sympathetic system has also been found to occur concurrently with a client’s significant insight (Kykyri et al., 2017) and in moments when the client recounted several difficult events and expressed disappointment (Avdi & Evans, 2020). These findings suggest that measuring physiological responses can enhance our understanding of the interactions occurring between client and therapist and facilitate our understanding of therapeutic processes (see Blanck et al., 2019). Thus, investigating the associations between physiological arousal and ongoing therapeutic dialog has the potential to provide insights into the emotions and meanings attached to the dialogic themes during psychotherapy sessions.
The Present Study: HRV as Indicator of Emotions and Meanings Behind the Words
We aimed to gain further knowledge on the added value of using RMSSD as a proxy for parasympathetic activation in understanding therapeutic experiences. The study was based on the idea that detecting subtle physiological changes during a therapy session may provide information about the emotional processes underlying the words and about the meanings attached to the ongoing dialog that cannot be accessed through observation or therapist self-reflection. The hypothesis tested was that RMSSDs reflect the physiological activity of the client and the psychotherapist and are related to the ongoing dialogue. Based on previous studies and the life situation of the client, we expected that despair and sadness would be seen as a decrease and the validation provided by the therapist as a rise in the client RMSSD.
Method
The Client
The client was a young Caucasian woman with a generalized anxiety disorder. She had been on disability pension since her adolescent years. Although she had good reflective skills and was very capable of expressing her thoughts verbally, her face was rather expressionless, as she controlled some of her emotions. The HRV and audio recordings were made when she had attended psychotherapy for about one and a half years in the private practice of the first author using integrative psychotherapy approach. The study was conducted with her approval, and she gave her informed consent. She read and commented on the manuscript. She listened to the audio recording together with the therapist and then discussed it in relation to the RMSSD profiles. However, due to her anxiety, she did not want to have video recordings, she feared she would be too aware of the recordings. A total of five sessions were HRV recorded, but no audio recorder was used during the first session in order not to put too much pressure on the client. The session selected for the present study was the first in which both HRV and audio recordings were used. Recently, an event in her immediate family had caused her increasing anxiety and intensified her feelings of hopelessness and meaninglessness. This manifested itself, inter alia, in increased images of how death would put her out of her misery. The therapy session analyzed in this study concerned the family event and the client’s emotions and thoughts related to it and to her relatives.
Data Collection and Analysis
Electrocardiograms (ECG) were recorded using two electrodes (Ag/AgCl, Ambu Neuroline 710) positioned under the collarbone on the right side of the body, and on the rib cage on the left side. The electrodes were connected to a Faros 180 ECG monitoring device, which acquired and stored the recordings at a sampling rate of 1,000 Hz (www.bittium.com). Before the start of the sessions, the Faros devices were synchronized using the Faros Manager program. Data downloaded from the Faros devices were checked and analyzed using the Kubios HRV Scientific 3.5.0 program (www.kubios.com). The program automatically removed recording artifacts, detected heartbeats, and performed HRV analysis. RMSSD is suitable for short measurement intervals (Shaffer & Ginsberg, 2017), and in the present study, we used an interval of one minute, that is, the RMSSDs of the heartbeats were calculated for consecutive 60-second periods as recommended in Chou et al. (2021). RMSSD is expressed in milliseconds; high readings indicate higher parasympathetic activity. The data were standardized by computing standard scores using the mean and standard deviation (SD) of the session separately for the client and the therapist. The time slots when either the client or therapist RMSSD changed over 1 SD were analyzed. We considered 1 SD to indicate a reliable change, as it contains the biggest 16% of the RMSSD changes. As we were interested in the themes of the dialogue rather than a nuanced moment-by-moment analysis of the interaction, a time window of at least 2 min was deemed appropriate to allow for meaningful themes to emerge in the dialogue without the constraint of containing multiple themes. Moreover, as the RMSSD could be increased only for part of the time during the one-minute period, a two-minute criterion was established as a reliable change in RMSSD. Four types of time slots fulfilled the preset criteria: (1) decreases in the client RMSSD, (2) rises in the client RMSSD, (3) rises in the therapist RMSSD, and (4) rises in both RMSSDs.
To ensure the fidelity of the content, the first author listened to the dialog between the client and the therapist several times. The following steps were taken collectively by debating and testing the ideas in a dialog between the authors. The main themes of the discussion were summarized in the following descriptions, and their relation to the RMSSD changes were analyzed qualitatively. The therapist had known the client for over a year, and this was reflected in her interpretations and comments during the dialog.
Results
Fig. 1 demonstrates both the client and the therapist RMSSDs over the session. Decreases and rises in the client RMSSD are indicated below and the rise in the therapist RMSSD above the profiles. As decreases and rises in the client and the therapist RMSSDs partly overlap, the descriptions of the dialogue do not form a chronological narrative.
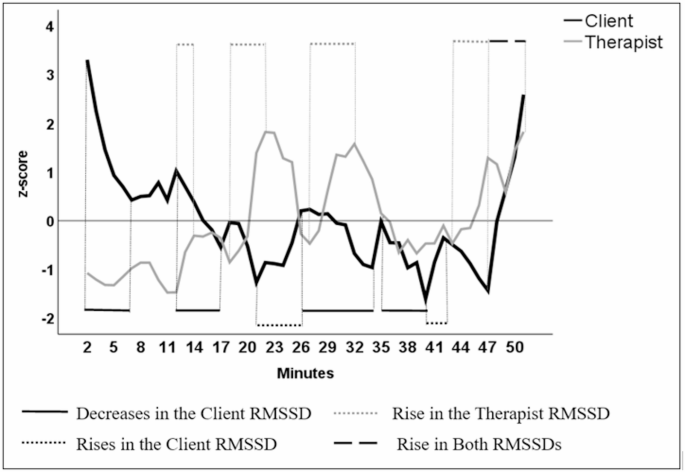
The client and the therapist RMSSDs over the session
Decreases in the Client RMSSD
There were four time slots with a clear decrease in the client RMSSD lasting more than 2 min, first occurring right at the beginning of the session (2–6 min) and the second soon following it (12–17 min). The third decrease occurred in the second half of the session (26–34 min) and was soon followed by the fourth decrease (35–40 min).
The First Decrease in the Client RMSSD (2–6 min)
At the beginning of the session, the client shared her unpleasant physical experiences (“somebody was drawing my head down” and “feeling of vomiting”) when expecting to meet and finally met her close relatives. She talked about her thoughts concerning these family relationships and the controversial feelings and emotions they evoked (e.g., guilt and bad conscience).
The Second Decrease in the Client RMSSD (12–17 min)
The client described her will to distance herself from her relatives and her will to stay away from their discussions to protect herself. She told about seeing her future as “empty,” as she had “dropped off.” She described how she felt that the past and the future were slipping away, as if she would be far away from a “distant river of life” and not be part of what was going on around her.
Toward the end of this time slot, the therapist RMSSD started to rise. At 16 min, the therapist noticed that the client was tearful and offered her handkerchiefs. Although the therapist did not say it aloud in the session, at this moment, she remembered the client’s earlier wishes to die. She thus interpreted the client’s present talk in the “wish to die” framework and noted “how sad the thoughts are” and how understandable it was that the client wanted to avoid these thoughts and emotions raised by the visit of the relatives. At 17 min, the therapist directed both the client’s and her own attention to the client’s bodily postures and expressions and expressed her observation that the client was holding her breath. The therapist guided the client to breathe in and sigh, which the client did, but according to the client, it did not feel emotionally helpful.
The Third Decrease in the Client RMSSD (26–34 min)
The client talked about her controversial close relationships, about not being able to change herself, and about her anger and grumpiness. At 27 min, the therapist asked how the client felt about the happy feelings expressed by other family members in relation to the family event she was talking about, and the client described her will not to take part in those feelings. The therapist validated this and proposed an interpretation that it was the client’s way to protect herself (and the therapist RMSSD was raised), but she also noted how this led to the client being and feeling an outsider to everything. The client further described her future as an outsider and how she cannot and will not change, although everything else changes.
At 30 min, the therapist said that she also became angry when thinking of how the recent family event had affected the client. At that point, a steeper decrease in the client RMSSD occurred. She sighed, and the therapist encouraged her to fortify the sigh and expressed how the client was probably experiencing a complex array of emotions, including sadness, desperation, and anger. The client agreed but called her feelings grumpiness rather than anger, which she saw as too strong a word. They also wondered whether it was more like disappointment, accusation, and guilt. At 32 min, the therapist asked the client about her possibility of finding secure or soothing images, which the client said was not possible now, except by avoiding situations and people. The client described her ways of regulating her anxiety, which occurred simultaneously with a short rise in her RMSSD.
The Fourth Decrease in the Client RMSSD (35–40 min)
The therapist suggested that the client was allowed to express her feelings and questioned whether her negative emotions were unacceptable. The client replied that her feelings, which she felt both unacceptable and too strong, caused her guilt and described how she sees herself as a “weak, wrong, bad, evil, jealous person.” (During this talk, the therapist RMSSD decreased.) The therapist said that it is understandable that the client cannot hold in her mind an image of herself as a bad person and simultaneously feel allowed to negative emotions. She also said that the client’s inner voice accusing her of her thoughts sounded very condemning, as the client’s emotions were extremely human. The client disagreed, saying that her emotions were too extreme and strong. The therapist validated and normalized the client’s emotions in light of the client’s life history, after which the client RMSSD increased.
Comments on the Decreases in the Client RMSSD
The common nominators of these periods of RMSSD decrease are threefold. First, they occurred as she described either her unpleasant physical experiences or her feelings and emotions, which she did not accept in herself. Second, moments of sadness could be recognized as the decreases occurred when the dialog concerned the client’s wishes to die and feelings of being an outsider. The third theme during these time slots was the client’s difficulties in receiving and accepting empathy or validation offered by the therapist or as it did not feel emotionally helpful.
Rises in the Client RMSSD
There were two time slots with a clear rise in the client RMSSD, the first occurring at 21–26 min and the second occurring at 40–43 min. There was also a third one, but as it occurred simultaneously with a rise in the therapist RMSSD, it will be described later.
The First Rise in the Client RMSSD (21–26 min)
Around 21 min later, the conversation turned to the client’s fears and desperation. The therapist described her understanding of these feelings using the client’s metaphor of “the distant river” and encouraged the client to think about whether there was any way for her to approach the river. The client pondered whether it was a question of will or a lack of means to do it. The therapist asked whether the opposite of the will was fear. The client further wondered to what extent it was fear and desperation but admitted that she had the will. The therapist provided an interpretation of the client’s situation and emotions, including her anger, within the framework of her history. The client corroborated this interpretation with words and sighs. At around 25 min, the client recognized herself as being “a bit angry” about the situation, and after that, a steep rise in her RMSSD occurred.
The Second Rise in the Client RMSSD (40–43 min)
At 40 min, after the client had talked about “guilt” and being a “weak, wrong, bad, evil person” and after having received validation of these feelings from the therapist, the therapist asked whether it would be possible for the client to interpret her feelings somehow other than being a bad person because of the feelings. The therapist shared her thoughts about how wrong it was that the client directed all the hatred toward herself and how sad it was. The client admitted that this was true but said that it was easier for her to be angry at herself and feel guilty than to be angry at others. She described how she showed her feelings to others by being “grumpy” at home, and even this gave her a guilty conscience; thus, it was better to direct her anger toward herself. The therapist validated the client’s feelings and the unfortunate circumstances of her life, which did not align with the client’s expectations. The therapist said that the current situation was sad, but neither of them knew what the future might hold. She reminded the client that she had not chosen to be in such a situation. However, the client explained how she thought she was to blame for her situation. Afterward, the client moved on to her earlier discourse of blaming herself for her thoughts and emotions (this co-occurred with a decrease in her RMSSD, however, this decrease was less than 1 SD).
Comments on the Rises in the Client RMSSD
There were two common nominators in these rises in the client RMSSD. On both occasions, she was able to name her condemnable or forbidden emotions and behavior, as she recognized being “a bit angry” and being “grumpy” at home. She could also stay with these emotions and reflect on them, and probably aimed to regulate them. On either occasion, she did not deny or reject the therapist’s interpretation of her situation, or the validation and empathy offered by the therapist.
Rise in the Therapist RMSSD
There were four time slots in which the therapist RMSSD showed clear rises. The first occurred at 12–14 min, the second at 18–22 min, the third at 27–32 min, and the last at 43–47 min. There was also a fifth one occurring simultaneously with a rise in the client RMSSD; this will be described later.
The First Rise in the Therapist RMSSD (12–14 min)
During this time slot, the therapist was hardly talking, as she was mainly listening to the client’s talk about her unpleasant physical experiences and her thoughts and feelings concerning her family.
The Second Rise in the Therapist RMSSD (18–22 min)
At 18 min, the client continued talking about her tearfulness last night and her thoughts about how everything was drifting away. Crying last evening had not felt comforting for her; it merely took her to her own space. The therapist validated the client’s emotions at 20 min. The client continued talking about her inability to be a good relative and how she felt that her failures were “being rubbed in her face.” After this, the therapist rephrased and interpreted the client’s thoughts and expressed her own sadness related to the situation. She encouraged the client to think about whether there were any ways in which the client could approach the “river of life”.
The Third Rise in the Therapist RMSSD (27–32 min)
The client talked about her thoughts of not being a good relative to a child who was soon to be born to the extended family. The therapist summarized previous topics and interpreted the client’s thoughts about distancing herself from others. They kept talking about the will and fear of being close to the relatives and the client’s belief that she was not able to change. At 30 min, the therapist said that she also became angry about what was going on in the client’s life. The client sighed heavily, and the therapist encouraged her to fortify it. While the client was doing this, the therapists talked about possible feelings of sadness, anger, and guilt inside the client by suggesting that these feelings needed to be let out. The therapist also validated the client’s feelings, which the client did not do.
The Fourth Rise in the Therapist RMSSD (43–47 min)
The client talked about how her situation was her own fault, blaming herself for her previous behavior and feeling incapable. The therapist replied by saying how cruel it sounded to blame the client’s younger self and called after self-compassion. The therapist encouraged the client to allow her to feel sorrow and listen to her tears. At 45 min, the therapist said that the sadness and the situation were not the client’s fault, and that the client was not bad; she repeated this phrase several times. Around this part of the session, there were long silences, but the therapist also talked quite a lot, describing the developmental process of the client, encouraging her to be self-compassionate and reminding the client how she can be proud of the work she has done.
Comments on the Rises in the Therapist RMSSD
There were two common features in the four time slots in which the therapist RMSSD rose. In the last three time slots, the therapist expressed her empathy to the client, and in the first one, she probably felt it, even though she did not express it, as she was only listening to the client. Alternatively, the therapist RMSSD rose in the first time slot as a reaction to the prolonged talk by the client and intensive listening while simultaneously preparing to reply. During the three time slots with the therapist’s empathy expressions, she talked a lot. It is plausible that it was the empathy felt by the therapist that mostly explained these rises. Interestingly, the client RMSSD did not rise simultaneously, despite the therapist’s expressions of empathy and validation. However, on three occasions (at 21, 34, and 37 min), a rise in the client RMSSD occurred either toward the end of the therapist’s speech and expression of understanding and empathy or soon after the therapist had stopped talking.
Rise in Both RMSSDs
Toward the end of the session, both the client and therapist RMSSDs were raised simultaneously; first, this was observed in the client (47–51 min) and then in the therapist (49–51 min). The therapist talked about whether there was a way for the client to defend against her inner voices, which were constantly claiming that the client was evil. The therapist also repeated her earlier remark that the client was not to blame, and that despite sadness, there were no reasons to feel guilty. The client said that she felt able to try to defend herself. The therapist told the client how punishing herself for her feelings felt cruel and wrong. The therapist also offered an interpretation that the client somehow felt rewarded for punishing herself, as if it were an absolution. She also reminded the client that accepting sadness and self-compassion needed rehearsal. Perhaps the empathy provided by the therapist was accepted by the client; the client teared up a little, which coincided with the time when her RMSSD was at its highest.
Comments on the Rises in Both RMSSDs
It is plausible that the therapist RMSSD mainly continued to rise as she interpreted and validated the client’s situation, that is, due to talk and empathy. It is probable that the empathy expressed by the therapist was finally received and accepted by the client at the end of the session, when she also teared up. Hence, it can be understood that the increases in the RMSSDs reflect both the shared understanding and emotions and the closure of the session, which may have allowed the emotion to finally be more freely expressed by the client.
Discussion
In this case study, we aimed to gain further knowledge of the added value of RMSSD as a proxy for parasympathetic activation in understanding therapeutic experiences and, more specifically, the emotions and meanings attached to the dialog. To achieve this goal, we examined the associations between the themes of the dialog and the RMSSDs of the client and the psychotherapist. The study showed that changes in the RMSSDs were logically related to the emotional content addressed in the conversations. This suggests the potential value of HRV indices (in this study RMSSD) as a tool in the search for understanding of clients’ experiences during psychotherapeutic interactions.
As expected, the decreases in the client RMSSD occurred when she was describing previously experienced sadness or unpleasant experiences. Thus, it appears that the client’s parasympathetic system became less active when the topics were such that it would be understandable for her to experience negative feelings. This is in line with previous studies demonstrating associations between high autonomic arousal and a patient’s strong emotions or an emphasis on negative emotions (Del Piccolo & Finest, 2018) and with studies showing association between negative affect and HRV reduction (Gullet et al., 2023; Sin et al., 2016).
Somewhat unexpectedly, decreases in the client RMSSD also occurred in moments when the psychotherapist expressed empathy or validated her experiences or emotions. This is in contrast with the assumption that empathy could increase the feeling of safety reflected in RMSSD rise (Petrocchi & Cheli, 2019) and with the view that the client’s feeling of being received and understood is associated with increase in parasympathetic activation (Deits-Lebehn et al., 2020). However, there is also evidence, albeit from non-psychotherapeutic contexts, that patients with high anxiety may show higher arousal during supportive conditions (Del Piccolo & Finset, 2018). Hence, decreases in the client RMSSD could be an indication that she was not able to accept empathy. That is, she did not feel like earning empathy, and she also indicated this during the fourth drop in her RMSSD by saying that her emotions were too extreme and strong. Based on her words and the RMSSD, it is plausible that the meanings the client attached to the psychotherapist’s words and expressions provoked her feelings of shame or inferiority, as she saw herself as unworthy of empathy, even though, she later said that the therapist’s validation and need for self-compassion were accurate.
The above-described moments can also be understood as instants of distance or strain between the client and the therapist, that is, alliance ruptures. This interpretation would be consistent with the findings from an interview context indicating that increased emotional distance between interviewer and respondent was associated with decreased skin conductance concordance and subjective ratings of perceived empathy (Marci & Orr, 2006). It also concords with the finding that identity blaming in a couple therapy session was accompanied by increased arousal (Päivinen et al., 2016), suggesting that sympathetic activation may increase when something that does not fit a person’s identity narrative is expressed.
The rise in the client RMSSD occurred when she named emotions and behavior that she regarded as condemnable and when she did not deny the psychotherapist’s interpretation, validation, or empathy. This finding suggests that the client found it somewhat reassuring to verbalize thoughts that caused guilt, which had previously been repressed. This would not have been apparent from the client’s words, nor could it have been observed and interpreted from her rather controlled and expressionless face. Interestingly, when the client herself later listened to the audio recordings with the psychotherapist, she noted that the strength of the valence of her emotions was not audible in her rather controlled and unnuanced voice. Hence, the RMSSD gave us a new understanding of the situation and the strength of her emotions at an embodied level, as observed in her physiological reactions.
The association between the naming of emotions and behavior that the client did not accept in her for the first time and the simultaneous rise in her RMSSD can be understood in terms of “sharing the emotional load” (Peräkylä et al., 2015). Perhaps by relying on the psychotherapist’s understanding, the client was able to transfer some of the emotional arousal associated with her controversial and guilt-provoking feelings to the therapist. This, of course, also requires feeling safe, which has been linked to parasympathetic activation (Deits-Lebehn et al., 2020; Petrocchi & Cheli, 2019). Furthermore, both moments were followed by a clear increase in the psychotherapist RMSSD, perhaps reflecting an instance of emotional co-regulation contributing to emotional and physiological stability for both the client and the psychotherapist (Butler & Randall, 2013). Thus, the rises in the client RMSSD, and those seen in the psychotherapist RMSSD, could also indicate the client’s efforts to adaptively regulate her emotions and the therapist’s efforts to encourage her to do so, and the related attentional and cognitive process (Luque-Casado et al., 2016; Thayer & Brosschot, 2005).
The psychotherapist RMSSD rose when listening to the client’s negative and self-blaming thoughts—that is, it rose when the psychotherapist probably felt empathy or actively processed the client’s discourse, as well as when the psychotherapist spoke for a longer period. Thus, it appears that the psychotherapist’s empathy and/or her own talk were responsible for the rise in her RMSSD on most occasions. However, rise did not occur on all occasions comprising longer periods of psychotherapist’s talk, suggesting that rise in her RMSSD cannot be explained solely by breathing related to talking. Interpreting the RMSSD rises as reflecting the therapist’s feelings of empathy or compassion is in concordance with previous studies indicating that heart rate decreases during empathizing (Himichi & Ohtsubo, 2020) and that the feeling of compassion is associated with heightened parasympathetic activity (Stellar et al., 2015). However, attentional focusing has also been associated with cardiac deceleration (Bradley, 2009), which is in line with the rise in the psychotherapist RMSSD while listening to the client at the beginning of the session.
The final rise in the client RMSSD (simultaneously with the psychotherapist) was probably associated with the client finally accepting empathy offered by the therapist and her feelings of safety, as well as feeling some degree of self-compassion, as it co-occurred with the client’s tearfulness. It is also plausible that awareness of the approaching end of the session may have facilitated the acceptance and expression of emotions. Nevertheless, it seems reasonable to interpret that the psychotherapist’s empathy, the client’s self-compassion, and the relief experienced after expressing forbidden and guilt-provoking emotions and behaviors contributed to the increase in parasympathetic activations at the end. This is in accordance with findings indicating increased parasympathetic activity when feeling safe (Petrocchi & Cheli, 2019), understood (Deits-Lebehn et al., 2020), experiencing therapeutic presence (Deits-Lebehn et al., 2020), and as a response to self-compassionate imaginary (Naismith et al., 2023), feelings of compassion (Stellar et al., 2015) and empathy (Deits-Lebehn et al., 2020). Thus, our findings from a clinical context can be interpreted cautiously to support Petrocchi and Cheli’s (2019) claim that HRV is associated with a sense of safety, derived from the ability to self-soothe during stress, which inhibits distress-related tendencies to fight or withdraw from suffering and facilitates engagement with suffering. It also concords with Deits-Lebehn et al.’s (2020) conclusion that therapeutic presence (i.e., feeling of being received, understood, and safe in therapy) is associated with clients’ parasympathetic activation.
As this was a single-case study involving only one psychotherapy session, which limits the generalizability of the findings, it must be considered preliminary. It is also worth remembering that during the complex and multifaceted psychotherapy dialog, the client may be responding to multiple internal and external cues that may not be apparent to either the client or the psychotherapist. Thus, the RMSSDs in the present study were bound to include stretches of non-emotional activity of the autonomic nervous system (e.g., cognitive processing, physical movement, respiratory pattern). Therefore, caution should be exercised when interpreting our findings, and straightforward causal inferences should be avoided, and, in the future, multiple indices should be used to gain more versatile data on the processes.
Another limitation is that only audio recording was used and that only the first author listened to and transcribed the content of the recording. Listening to the tapes was restricted to the therapist to respect and protect the privacy of the client, who the therapist felt was in too vulnerable a position to ask for permission for others to listen to the recordings. Then again, the client herself contributed to the interpretations of the contents and meanings of the discussion as she read the manuscript and listened the tape together with the therapist. In a similar vein, to protect the privacy of the client, no precise turn-by-turn description of the dialog is provided. However, our research question did not require a detailed moment-by-moment analysis of the dialog, as we wanted to focus on broader themes.
The present study’s strength lies in the fact that it was conducted within a natural, everyday clinical context, as opposed to those conducted in a laboratory, thereby ensuring the ecological validity of the study. While the implementation of supplementary data collection methodologies, like video recordings or simulated recall interview after the session, would have furnished a more comprehensive understanding, their utilization in clinical practice is not as feasible as in studies conducted in a research context. This underscores the notion that conducting psychophysiological research, and indeed any other form of research, during actual psychotherapy in a clinical setting poses significant challenges. The fundamental objective of psychotherapy, which is the client’s well-being, invariably takes precedence.
Despite the limits, it can be concluded that RMSSDs gave clinically meaningful information, especially regarding the client’s possible experiences when the therapist sought to provide empathy and validation as well as regarding the strength of her emotions, which could not be interpreted from her voice or her facial expression. More research is needed to better understand the relational dynamics contributing to changes in both clients’ and therapists’ HRVs. In the future, research could enlighten us about the value of incorporating online HRV biofeedback into clinical encounters (see Lehrer et al., 2020), for example, by informing whether the client’s activation level remains within the window of tolerance, as such immediate feedback could inform the therapist’s actions. Incorporating psychophysiological or other embodied information could also have added value for psychotherapy research (Lehrer, 2024), for example, by informing us how to fine-tune therapy processes to better suit clients who are less verbally fluent (Nyman-Salonen et al., 2022). Furthermore, to gain a better understanding of the therapeutic experiences, it is recommended to adopt a turn-by-turn micro-analytic approach that examines the dialogic processes throughout the session rather than focusing on specific isolated moments. This approach would allow for a more comprehensive analysis of interaction dynamics.
Data Availability
No datasets were generated or analysed during the current study.
References
-
Avdi, E., & Evans, C. (2020). Exploring conversational and physiological aspects of psychotherapy talk. Frontiers in Psychology, 11, 591124. https://doi.org/10.3389/fpsyg.2020.591124
-
Balzarotti, S., Biassoni, F., Colombo, B., & Ciceri, M. R. (2017). Cardiac vagal control as a marker of emotion regulation in healthy adults: A review. Biological Psychology, 130, 54–66. https://doi.org/10.1016/j.biopsycho.2017.10.008
-
Blanck, P., Stoffel, M., Bents, H., Ditzen, B., & Mander, J. (2019). Heart rate variability in individual psychotherapy: Associations with alliance and outcome. The Journal of Nervous and Mental Disease, 207(6), 451–458. https://doi.org/10.1097/NMD.0000000000000994
-
Bradley, M. M. (2009). Natural selective attention: Orienting and emotion. Psychophysiology, 46(1), 1–11. https://doi.org/10.1111/j.1469-8986.2008.00702.x
-
Butler, E. A., & Randall, A. K. (2013). Emotional coregulation in close relationships. Emotion Review, 5(2), 202–210. https://doi.org/10.1177/1754073912451630
-
Chou, E. F., Khine, M., Lockhart, T., & Soangra, R. (2021). Effects of Ecg data length on heart rate variability among young healthy adults. Sensors (Basel, Switzerland), 21(18), 6286. https://doi.org/10.3390/s21186286
-
Deits-Lebehn, C., Baucom, K. J., Crenshaw, A. O., Smith, T. W., & Baucom, B. R. (2020). Incorporating physiology into the study of psychotherapy process. Journal of Counseling Psychology, 67(4), 488. https://doi.org/10.1037/cou0000391
-
Del Piccolo, L., & Finset, A. (2018). Patients’ autonomic activation during clinical interaction: A review of empirical studies. Patient Education and Counseling, 101(2), 195–208. https://doi.org/10.1016/j.pec.2017.08.007
-
Grossman, P., & Taylor, E. W. (2007). Toward Understanding respiratory sinus arrhythmia: Relations to cardiac vagal tone, evolution and biobehavioral functions. Biological Psychology, 74(2), 263–285. https://doi.org/10.1016/j.biopsycho.2005.11.014
-
Gullett, N., Zajkowska, Z., Walsh, A., Harper, R., & Mondelli, V. (2023). Heart rate variability (HRV) as a way to understand associations between the autonomic nervous system (ANS) and affective States: A critical review of the literature. International Journal of Psychophysiology, 192, 35–42. https://doi.org/10.1016/j.ijpsycho.2023.08.001
-
Himichi, T., & Ohtsubo, Y. (2020). An inverted U-shaped relationship between heart rate deceleration and empathic emotions. Biological Psychology, 150, 107828. https://doi.org/10.1016/j.biopsycho.2019.107828
-
Kykyri, V. L., Karvonen, A., Wahlström, J., Kaartinen, J., Penttonen, M., & Seikkula, J. (2017). Soft prosody and embodied attunement in therapeutic interaction: A multimethod case study of a moment of change. Journal of Constructivist Psychology, 30(3), 211–234. https://doi.org/10.1080/10720537.2016.1183538
-
Kykyri, V. L., Nyman-Salonen, P., Tschacher, W., Tourunen, A., Penttonen, M., & Seikkula, J. (2024).: Exploring the role of emotions and conversation content in interpersonal synchrony: A case study of a couple therapy session. Psychotherapy Research,1–7.https://doi.org/10.1080/10503307.2024.2361432
-
Laborde, S., Mosley, E., & Thayer, J. F. (2017). Heart rate variability and cardiac vagal tone in Psychophysiological research–recommendations for experiment planning, data analysis, and data reporting. Frontiers in Psychology, 8, 213. https://doi.org/10.3389/fpsyg.2017.00213
-
Laitila, A., Vall, B., Penttonen, M., Karvonen, A., Kykyri, V. L., Tsatsishvili, V., & Seikkula, J. (2019). The added value of studying embodied responses in couple therapy research: A case study. Family Process, 58(3), 685–697. https://doi.org/10.1111/famp.12374
-
Lane, R. D., Subic-Wrana, C., Greenberg, L., & Yovel, I. (2022). The role of enhanced emotional awareness in promoting change across psychotherapy modalities. Journal of Psychotherapy Integration, 32(2), 131–150. https://doi.org/10.1037/int0000244
-
Lehrer, P. (2024). The importance of including Psychophysiological methods in psychotherapy. Applied Psychophysiology and Biofeedback, 1–20. https://doi.org/10.1007/s10484-024-09667-w
-
Lehrer, P., Kaur, K., Sharma, A., Shah, K., Huseby, R., Bhavsar, J., & Zhang, Y. (2020). Heart rate variability biofeedback improves emotional and physical health and performance: A systematic review and meta-analysis. Applied Psychophysiology and Biofeedback, 45, 109–129. https://doi.org/10.1007/s10484-020-09466-z
-
Luque-Casado, A., Perales, J. C., Cárdenas, D., & Sanabria, D. (2016). Heart rate variability and cognitive processing: The autonomic response to task demands. Biological Psychology, 113, 83–90. https://doi.org/10.1016/j.biopsycho.2015.11.013
-
Marci, C. D., & Orr, S. P. (2006). The effect of emotional distance on psychophysiologic concordance and perceived empathy between patient and interviewer. Applied Psychophysiology and Biofeedback, 31, 115–128.
-
Marci, C. D., Ham, J., Moran, E., & Orr, S. P. (2007). Physiologic correlates of perceived therapist empathy and social-emotional process during psychotherapy. The Journal of Nervous and Mental Disease, 195(2), 103–111.
-
Mylona, A., Avdi, E., & Paraskevopoulos, E. (2023). Alliance rupture and repair processes in psychoanalytic psychotherapy: Multimodal in-session shifts from momentary failure to repair. Therapeutic failures in psychotherapy (pp. 98–125). Routledge.
-
Naismith, I., Scheiber, O., Rodriguez, C. S. G., D., & Petrocchi, N. (2023). Physiological response to self-compassion versus relaxation in a clinical population. Plos One, 18(2), e0272198. https://doi.org/10.1371/journal.pone.0272198
-
Nyman-Salonen, P., Kykyri, V. L., & Penttonen, M. (2022). Challenges and added value of measuring embodied variables in psychotherapy. Frontiers in Psychiatry, 13, 1058507. https://doi.org/10.3389/fpsyt.2022.1058507
-
Päivinen, H., Holma, J., Karvonen, A., Kykyri, V. L., Tsatsishvili, V., Kaartinen, J., & Seikkula, J. (2016). Affective arousal during blaming in couple therapy: Combining analyses of verbal discourse and physiological responses in two case studies. Contemporary Family Therapy, 38, 373–384. https://doi.org/10.1007/s10591-016-9393-7
-
Peräkylä, A., Henttonen, P., Voutilainen, L., Kahri, M., Stevanovic, M., Sams, M., & Ravaja, N. (2015). Sharing the emotional load: Recipient affiliation calms down the storyteller. Social Psychology Quarterly, 78(4), 301–323. https://doi.org/10.1177/0190272515611054
-
Petrocchi, N., & Cheli, S. (2019). The social brain and heart rate variability: Implications for psychotherapy. Psychology and Psychotherapy: Theory Research and Practice, 92(2), 208–223. https://doi.org/10.1111/papt.12224
-
Pham, T., Lau, Z. J., Chen, S. A., & Makowski, D. (2021). Heart rate variability in psychology: A review of HRV indices and an analysis tutorial. Sensors (Basel, Switzerland), 21(12), 3998. https://doi.org/10.3390/s21123998
-
Porges, S. W. (2022). Polyvagal theory: A science of safety. Frontiers in Integrative Neuroscience, 16, 871227. https://doi.org/10.3389/fnint.2022.871227
-
Shaffer, F., & Ginsberg, J. P. (2017). An overview of heart rate variability metrics and norms. Frontiers in Public Health, 5, 258. https://doi.org/10.3389/fpubh.2017.00258
-
Sin, N., Sloan, R., McKinley, P., & Almeida, D. (2016). Linking daily stress processes and laboratory-based heart rate variability in a National sample of midlife and older adults. Psychosomatic Medicine, 78(5), 573–582. https://doi.org/10.1097/PSY.0000000000000306
-
Smith, R., Thayer, J. F., Khalsa, S. S., & Lane, R. D. (2017). The hierarchical basis of neurovisceral integration. Neuroscience & Biobehavioral Reviews, 75, 274–296. https://doi.org/10.1016/j.neubiorev.2017.02.003
-
Stellar, J. E., Cohen, A., Oveis, C., & Keltner, D. (2015). Affective and physiological responses to the suffering of others: Compassion and vagal activity. Journal of Personality and Social Psychology, 108(4), 572. https://doi.org/10.1037/pspi0000010
-
Thayer, J., & Brosschot, J. (2005). Psychosomatics and psychopathology: Looking up and down from the brain. Psychoneuroendocrinology, 30, 1050–1058. https://doi.org/10.1016/j.psyneuen.2005.04.014
-
Thomas, B. L., Claassen, N., Becker, P., & Viljoen, M. (2019). Validity of commonly used heart rate variability markers of autonomic nervous system function. Neuropsychobiology, 78(1), 14–26. https://doi.org/10.1159/000495519
-
Tschacher, W., & Meier, D. (2020). Physiological synchrony in psychotherapy sessions. Psychotherapy Research, 30(5), 558–573. https://doi.org/10.1080/10503307.2019.1612114
-
Wu, Y., Gu, R., Yang, Q., & Luo, Y. J. (2019). How do amusement, anger and fear influence heart rate and heart rate variability? Frontiers in Neuroscience, 13, 1131. https://doi.org/10.3389/fnins.2019.01131
Acknowledgements
We would like to express our sincere gratitude to the client for her willingness to participate in psychophysiological measures as part of her psychotherapy and for her cooperation in the interpretation of the data.
Funding
Open Access funding provided by University of Jyväskylä (JYU).
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
Reprints and permissions
About this article
Cite this article
Aro, T., Kykyri, VL. & Penttonen, M. Exploring the Added Value of Heart Rate Variability in Assessing Psychotherapeutic Experience: A Single Case Study. J Contemp Psychother (2025). https://doi.org/10.1007/s10879-025-09680-y
- Accepted
- Published
- DOI https://doi.org/10.1007/s10879-025-09680-y
Keywords
- Psychotherapy dialog
- Case study
- Heart rate variability
- Parasympathetic activation