Article Content
Introduction
The aging of the global population brings with it complex challenges for public health, particularly concerning the mental health (MH) of older adults (OAs), as disorders such as depression and anxiety are among the leading causes of disability and reduced quality of life (Vigo et al., 2016; GBD 2017 Disease and Injury Incidence and Prevalence Collaborators, 2018). The prevalence of these disorders, which are among the most common causes of years lived with disability, is particularly high in Brazil (Murray et al., 2015). Aging, as a natural phase of life, involves changes in cognitive processing and may increase individuals’ susceptibility to both physical and MH challenges (Petrova & Khvostikova, 2021). In this context, the concept of healthy aging goes beyond the mere absence of disease, also encompassing psychological and social factors such as resilience, which are crucial for adapting to life transitions and maintaining emotional well-being (Moreno-Agostino et al., 2022; Southwick et al., 2005; Beutel et al., 2010).
Resilience, described as a mechanism that helps individuals recover and restore their equilibrium to pre-stress levels (Smith et al., 2008, 2010), emerges as a protective factor closely associated with improved physical and mental well-being in OAs (da Silva-Sauer et al., 2021b). Studies suggest that individuals with high resilience tend to exhibit fewer depressive symptoms when confronted with stress-inducing situations (da Silva-Sauer et al., 2021c; Moreno-Agostino et al., 2022), highlighting its role in fostering MH. Specifically, resilience has been linked to better quality of life and lower levels of mental distress, such as depression and anxiety, making it a central factor in promoting mental well-being as individuals age (Ávila et al., 2017). Moreover, factors such as religiosity and physical activity (PA) play essential roles in supporting the MH of OAs by providing emotional support and reducing symptoms of anxiety and depression (Roh et al., 2015; Southwick & Charney, 2012). Thus, when reflecting on healthy aging, it is important to consider how these factors interact to enhance MH and quality of life as individuals age.
Religion, defined as an organized system of beliefs, practices, rituals, and symbols that facilitates an approach to the sacred or transcendent (Koenig et al., 2001), has evolved to include positive spirituality, an aspect often overlooked in traditional aging models (Koenig, 2009). OAs are more likely to rely on religious and spiritual resources than younger individuals when seeking meaning in life and coping with challenges, especially in stressful situations (Lee & Zhang, 2018). These resources provide important coping mechanisms that support the mental and physical well-being of OAs (Carver & Buchanan, 2016; Li & Wang, 2022). Active participation in religious practices, such as attending services or engaging in rituals, can enhance this support by encouraging healthy behaviors, offering coping strategies, and fostering social connections during difficult times (Lucchetti et al., 2022). Research highlights that religious involvement not only mitigates the effects of illness and stress but also promotes better physical health by fostering supportive social networks and encouraging healthy behaviors (Lee, 2007; Oman & Syme, 2018).
Pargament et al. (2001) suggested that positive religiosity may moderate the relationship between resilience and mental well-being. While it may not be directly linked to resilience, positive religiosity can complement coping strategies by offering a belief system that helps individuals navigate life’s challenges in a more constructive way (Surzykiewicz et al., 2022). In this regard, religiosity acts as a “buffer” against stress, enhancing mental well-being through spiritual support, a sense of belonging to a religious community, and the belief in a greater purpose (Pargament et al., 2000, 2001).
Engaging in regular PA has well-established benefits for mental well-being, psychological resilience, and overall health (Wu et al., 2023). Studies show that PA improves resilience, helping individuals manage stress and enhancing their quality of life (Feil et al., 2021; Neumann et al., 2022). A longitudinal study tracking OAs over four years shows a positive relationship between consistent PA and resilience (Ávila et al., 2022). Additionally, the intensity of exercise is emphasized as significant, with preferred intensity levels sufficient to enhance resilience and quality of life (Lancaster & Callaghan 2022).
This study integrates the vulnerability-stress model (Ingram & Luxton, 2005) with Richardson’s (2002) concept of “biopsychospiritual homeostasis” to examine how resilience, PA, and religiosity interact to influence MH in Brazilian OAs. The vulnerability-stress model highlights how resilience protects against stressors, focusing on the interaction between individual vulnerabilities and external stress. The biopsychospiritual homeostasis concept views resilience as a dynamic balance between physical, psychological, and spiritual factors, with PA and religiosity supporting this equilibrium. Religiosity offers a system of beliefs to manage emotional challenges, while PA contributes to physical and psychological resilience. This study seeks to address this gap by exploring the interaction between resilience, PA, and religiosity within the biopsychospiritual framework in a large sample of community-dwelling OAs from the Northeast states of Brazil. By integrating these models, we aim to provide new insights into how resilience acts as a protective factor for MH in aging.
Our hypothesis suggests that OAs with higher resilience, active religious participation, and greater PA engagement will have better MH. Conversely, OAs with lower resilience, less religious participation, and lower PA involvement will show weaker or no such relationship. These findings aim to guide strategies for promoting MH in OAs, highlighting the role of resilience in successful aging and the potential influence of religiosity on positive outcomes.
Method
Participants
The study included a sample of 1001 community-dwelling older adults (OAs) aged 60 to 101 years (M = 68.6, SD = 6.9). Inclusion criteria were: (1) aged 60 or older (as per the World Health Organization’s classification for OAs in developing countries); and (2) cognitive intactness to understand and respond to the questions. All participants were in satisfactory general physical and mental health and had the autonomy to complete the survey. Informed consent was obtained from all participants before enrollment.
Measures
Sociodemographic Questionnaire
This questionnaire consisted of structured multiple-choice questions aimed at gathering the following participant profile information: age, gender, self-declared race/ethnic and years of education.
Physical Activity and Religiosity
To obtain data on PA, participants were asked, “Do you engage in walking or other routine physical exercises?” (e.g., walking for at least 15 min a day, at least twice a week), with the response options: 1 = No; 2 = Yes, one to two times per week; and 3 = Yes, three times or more per week. This PA measure aligns with current guidelines on moderate activity for OAs (Cunningham et al., 2020). The response categories of “1–2 times per week” and “3 times or more per week” reflect emerging evidence on the health benefits of even modest physical activity. To acquire data on religiosity, participants were asked, “Do you consider yourself a religious person?” with response options: 1 = Yes; 2 = No. This straightforward measure of religiosity reflects intrinsic religiosity, as discussed by Koenig and Büssing (2010), and captures the psychological aspect of religiosity related to well-being (Laurencelle et al., 2002).
Physical Activity and Religiosity Index (PaRI)
This is a combined six-level variable created by categorizing participants based on their levels of physical activity (PA) and religiosity. The PaRI serves as a moderator in the analysis, with the following six conditions: (1) religious participants who do not engage in physical activity, (2) religious participants who engage in physical activity up to twice a week, (3) religious participants who engage in physical activity three or more times per week, (4) non-religious participants who do not engage in physical activity, (5) non-religious participants who engage in physical activity up to twice a week, and (6) non-religious participants who engage in physical activity three or more times per week. By combining religiosity and physical activity into a single index, this approach allows for a nuanced examination of how these factors interact in relation to mental health outcomes.
Resilience
The Brief Resilience Scale (Smith et al., 2008) was used to assess an individual’s ability to recover from a stressful event. It consists of six questions, with items 1, 3, and 5 worded positively and items 2, 4, and 6 worded negatively. Responses were scored as follows: 1 = Strongly disagree; 2 = Disagree; 3 = Neutral; 4 = Agree; 5 = Strongly agree. The Brazilian version of the BRS (BRS-B) was validated by da Silva-Sauer et al. (2021a), with adequate internal consistency (ω = 0.79) in studies with OAs. Individual scores on the BRS-B can range from 6 to 30, with higher scores indicate greater resilience reserves. Cronbach’s alpha for this instrument in this study was 0.70, indicating acceptable internal consistency.
Perceived Stress
Perceived stress was measured using the Perceived Stress Scale (PSS; Cohen et al., 1983), specifically the 10-item version (PSS-10), validated for Brazilian OAs (Luft et al., 2007; α = 0.82). Participants rated items on a 5-point scale: 0 = Never; 1 = Almost never; 2 = Sometimes; 3 = Fairly often; 4 = Very often. Higher scores indicate higher perceived stress, with total scores ranging from 0 to 40. Cronbach’s alpha for the PSS in this study was 0.82, indicating good internal consistency.
Mental Health
Depressive and anxiety symptoms were assessed using the Hospital Anxiety and Depression Scale (HADS; Zigmond & Snaith, 1983). This scale consists of 14 items, with seven for anxiety (HADS-A, α = 0.84) and seven for depression (HADS-D, α = 0.83). Participants responded on a 4-point scale: 0 to 3, with total scores for each subscale ranging from 0 to 21. Higher scores indicate greater symptoms of anxiety and depression. The HADS was validated for Brazilian OAs (Botega et al., 1995). Cronbach’s alpha for the total score in this study was 0.84, indicating excellent internal consistency.
Procedure
The study employed a cross-sectional design to examine the interaction effects of resilience, PA, and religiosity on the MH of OAs. Specifically, the analysis investigated whether different levels of PA and religiosity moderated the association between resilience and symptoms of depression and anxiety. Data were collected at a single time point, enabling the assessment of relationships among these variables in the context of MH.
Data collection was conducted across multiple locations in three states in the Northeast region of Brazil: Paraíba (Cabedelo, Itapororoca, and João Pessoa), Pernambuco (Ipojuca and Recife), and Rio Grande do Norte (Ceará-Mirim) using a non-probabilistic convenience sampling method. Trained researchers approached individuals directly in public and community settings such as parks, health centers, and recreational areas, aiming to ensure the inclusion of community-dwelling OAs.
Each participant completed the survey individually in a single session lasting approximately 15 min. The order of administration was standardized for all participants, beginning with the sociodemographic questionnaire, followed by assessments of physical activity and religiosity, and concluding with the BRS-B, the PSS, and the HADS.
Ethical Approval was obtained from the Research Ethics Committee of the Júlio Muller University Hospital (Approval No. 106/CEP-HUJM/2011). All participants provided written informed consent in accordance with Resolution No. 466/12 of the Brazilian National Health Council.
Data Analysis
Descriptive statistics (means, standard deviations, frequencies, and percentages) were calculated for all measures. Cronbach’s alpha was computed to evaluate internal consistency for each scale. A one-way ANOVA was performed to examine the effects of different moderator conditions on key variables. A simple moderation model (Process Model 1) was employed to investigate the interaction effects of resilience (X), the PaRI (W), and perceived stress (Z) on mental health (Y), measured by the HADS total score. Covariates included gender, age, race/ethnicity, and years of education. The model is depicted in Fig. 1. Moderation analysis was conducted using the PROCESS macro for SPSS (Hayes, 2018), with 10,000 bootstrap samples to establish 95% confidence intervals.
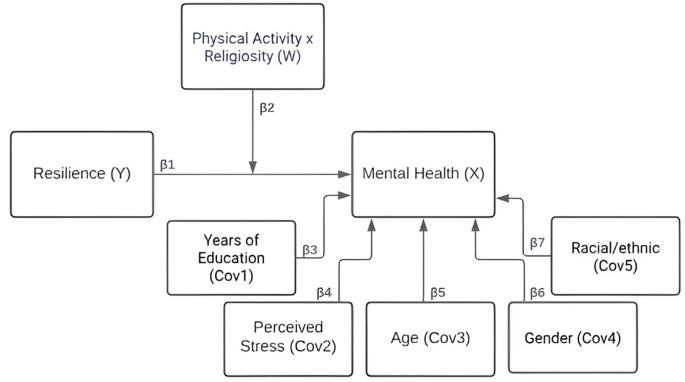
Model
Note: In the model: X = independent variable; W = moderator; Y = dependent variable; Cov = covariate
All statistical analyses were conducted using IBM SPSS version 25 (IBM, 2017), with a significance level set at p <.05.
Results
The sample consists of 57.5% females, 47.7% self-identifying as White, and a mean of 9.4 years of education (SD = 5.2). Table 1 presents the variations in outcomes across different moderator conditions.
The results revealed significant differences in key variables across the various conditions. Particularly noteworthy is Condition 3 (“Religious and engage in PA 3 or more times per week”), where participants showed higher levels of education and lower HADS total scores, indicating better MH compared to other conditions. Additionally, Condition 3 demonstrated notably higher resilience scores and lower perceived stress levels compared to several other conditions, suggesting that individuals who are religious and engage in regular physical activity tend to exhibit greater resilience. This implies a potential protective effect of religious engagement and PA on stress levels. Conversely, Condition 4, labeled “Not religious and does not engage in PA”, displayed the highest scores in HADS and PSS, ranking among the lowest in BRS-B, and also reported the lowest level of education among the conditions. Notably, age (years) did not show significant differences across conditions, indicating that age was consistent regardless of the varying combinations of religious affiliation and PA levels among the participants.
Moderation
The moderation analyses indicated that the overall model was statistically significant (R² = 0.523; MSE = 19.9; F(16, 979) = 67.29; p <.001), suggesting that the interaction between the independent variable (resilience) and the moderator (PaRI), while controlling for covariates, significantly influenced the MH of AOs, accounting for a substantial proportion of its variability. Furthermore, the specific interaction effect between resilience and PaRI, representing the combined influence of PA and religiosity, was also statistically significant (F(5, 979) = 2.50; p <.01), yielding a significant incremental change in explained variance for MH (ΔR² = 0.0061).
Table 2 reports the estimated effects of resilience on MH across different combinations of PA and religiosity levels. These effects are illustrated in Fig. 2. The results indicate that, among individuals engaging in PA three or more times per week, the association between resilience and MH was not statistically significant (p >.05). As shown in Fig. 2, this is reflected in the flat slope of the lines, represented by triangles and squares, suggesting that MH remained relatively stable across varying levels of resilience in these subgroups.
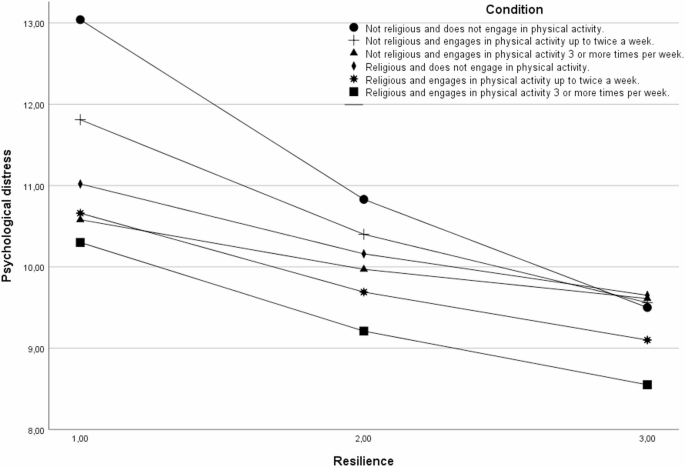
Variation in mental health by different levels of resilience in conditions of religious and physical activity. Note. The Y-axis represents levels of psychological distress, as measured by the Hospital Anxiety and Depression Scale (HADS), with higher scores indicating greater severity of anxiety and depression symptoms—reflecting poorer mental health. The X-axis represents resilience, assessed using the Brief Resilience Scale (BRS), where higher scores denote a greater capacity to recover from adversity. On the resilience scale, a score of 1 corresponds to low resilience, 2 to moderate resilience, and 3 to high resilience
In contrast, conditions involving individuals who do not engage in PA or who do so infrequently (up to twice a week) exhibited significant effects of resilience on MH. For individuals who reported no engagement in PA, resilience had the strongest negative effect (β = -0.44, p <.01), indicating substantial variation in MH as a function of resilience levels. Among those engaging in PA up to twice per week, the effect was also significant but of moderate magnitude (β = -0.25, p <.01), reflecting a weaker, yet still meaningful, association compared to the no-PA group.
These effects are clearly illustrated in Fig. 2, where marked differences in MH are observed between low and high levels of resilience, particularly within the low-activity subgroups. This pattern suggests that resilience plays a more prominent role in shaping MH outcomes when physical activity is absent or limited.
Although the interaction between resilience and the combined moderator (PaRI) was statistically significant, its practical contribution to explaining variance in MH was limited. Specifically, the interaction accounted for an additional 1% of the variance (ΔR² ≈ 0.01), indicating a small but significant moderation effect. Nevertheless, the overall model explained 52.38% of the variance in MH, which represents a substantial proportion. Thus, while the interaction term improved the model fit, its incremental explanatory power was relatively modest.
Discussion
This study examined the relationship between resilience, PA, and religiosity as protective factors for the MH of community-dwelling OAs. The findings showed a significant interaction among these variables concerning the MH. Specifically, the association between resilience and MH varied across different levels of the variable representing the interaction between PA and religiosity in OAs studied.
OAs groups engaging in higher weekly frequencies of PA showed significantly higher levels of resilience. These findings are consistent with previous research suggesting that resilience plays an essential role in promoting consistent exercise patterns, even in the face of common physical or emotional challenges associated with ageing, such as injury, vision problems or loneliness (Satariano et al., 2000). Importantly, resilient OAs show a greater propensity to engage in PA compared to their non-resilient counterparts (Perna et al., 2012). This observation highlights the potential efficacy of resilience as a strategic approach to mitigate the decline in exercise frequency commonly observed in the ageing population.
The results also suggest that engaging in PA three or more times per week had the greatest benefit for MH. OAs in this frequency group exhibited higher resilience, lower stress levels, and better MH overall, regardless of their level of resilience. This finding supports previous research indicating that frequent PA, at least three times a week, can significantly enhance the mental and social well-being of OAs (Rugbeer et al., 2017). This positive influence is attributed to the increased release of hormones like catecholamines, vasopressin, β-endorphin, dopamine, and serotonin following PA, which have relaxing effects and help alleviate anxious and depressive symptoms (Catalan-Matamoros et al., 2016).
The moderation analysis showed that the resilience significant influenced the MH of OAs who were neither religious nor engaged in PA. Resilience counteracted the potential negative effects of the absence of PA and non-religiosity, contributing to better MH scores for these OAs (as indicated by low scores on the HADS scale). These findings support previous studies demonstrating resilience as a protective factor for psychological health in aging individuals (da Silva-Sauer et al., 2021b; Moreno-Agostino et al., 2022) and suggest that promoting resilience may benefit the MH of non-religious individuals who do not engage in weekly physical exercise.
In groups where OAs identify as religious, religiosity can complement resilience as a spiritual resource. Religion, similar to resilience, plays a significant role in coping with adversity and managing stress (Talik & Skowroński, 2018). Religiosity provides mechanisms such as cognitive reappraisal, a sense of security, support, and perseverance in the face of stressful situations, serving as an active emotional regulation strategy (Dolcos et al., 2021). While OAs engaging in PA 1 to 2 times a week already experience benefits for MH, a stronger relationship was found in groups engaging in PA 3 times or more per week. PA can enhance resilience by improving the functioning of the nervous system, including top-down cognitive control, as well as behavioral and emotional self-regulation (Ho et al., 2015). This enhancement helps individuals become more resilient to the emotional effects of acute stress (Childs & de Wit, 2014), contributing to resilience development.
Our findings align with Richardson’s biopsychospiritual theory of resilience (Richardson, 2002), and suggest that religiosity and PA are important in promoting resilience and MH in OA. Religiosity offers a system of beliefs and values that assist individuals in addressing emotional challenges through religious coping (Dolcos et al., 2021), providing a sense of purpose and hope beneficial for MH in later life (Peres et al., 2007). In turn, regular PA strengthens physical health, helping prevent diseases such as hypertension, osteoporosis, heart attacks, and psychological factors such as stress, anxiety, and depression (Scolese et al., 2019). It also promotes emotional resilience (Ávila et al., 2022), providing resources for better physical and psychological well-being in OAs. Both factors are essential for individuals to adapt and recover from adversity, as pointed out by the biopsychospiritual theory of resilience, and our study demonstrates that PA and religion act as important moderators, influencing how resilience influences MH of OAs. Resilient OAs may benefit from both PA and participation in religious activities, while those with lower resilience may experience a more pronounced increase in MH when engaging in at least one of these practices.
We acknowledge that other aspects related to religiosity and PA could be implicated in this context. For instance, social support through participation in religious groups (Malone & Dadswell 2018) and regular PA (Smith et al., 2017) facilitates significant social networks, interactions, bonds, and a sense of belonging. Additionally, both religiosity (Malone & Dadswell 2018) and PA (Rugbeer et al., 2017) contribute to active and busy lifestyles, providing purpose and meaning, reducing stress through endorphin release, and promoting healthy lifestyles, resulting in better MH in OAs (Mikkelsen et al., 2017). However, these variables were not controlled for, indicating the need for future studies including them in the model.
Limitations and Implications of the Study
Our study presents several limitations that should be taken into account. Firstly, we assessed only the frequency of PA without considering important dimensions such as intensity (e.g., duration, level of effort) or type (e.g., aerobic vs. anaerobic exercise). Future studies should address this limitation by incorporating more comprehensive and multidimensional measures of physical activity. Secondly, religiosity was measured solely through participants’ self-reported perceptions, without collecting additional information on religious beliefs, practices, or affiliations. Further research could adopt a more nuanced approach, exploring dimensions such as spirituality, religious denomination, and the frequency or nature of religious practices. Thirdly, we did not assess the use of psychotropic medication, such as anxiolytics or antidepressants, which may have influenced participants’ levels of psychological distress. The inclusion of medication-related variables in future studies would help to better isolate the effects of resilience and the moderator variables on mental health outcomes. Moreover, although the interaction between resilience and the combined moderator (PaRI) was statistically significant, the effect size was modest, possibly due to characteristics of the sample or the way the moderator variables were coded. Limited variability in these variables may have led to range restriction, thereby reducing the potential to detect stronger interaction effects. Future studies could consider alternative operationalizations of moderator constructs or recruit more heterogeneous samples to increase variability. Fourthly, the use of a convenience sampling method may have limited the representativeness of the sample. As a result, the findings should be interpreted with caution, as they may not fully reflect the diversity of MH outcomes and behavioral patterns present in the broader population of OAs. Future research should consider employing probabilistic or stratified sampling techniques to enhance the external validity and generalizability of the results. Finally, due to the cross-sectional nature of the study, causal inferences cannot be drawn. Longitudinal studies are warranted to examine whether physical activity exerts a positive influence on OAs’ MH, or conversely, whether better mental health promotes greater engagement in PAs.
The theoretical implications of the results support the need to further explore these interactions to better understand their interrelationships and their impact on the MH of OAs living in community settings. Concurrently, the results highlight the importance of integrating resilience, consistent PA, and religiosity into health interventions and programs targeted at the elderly population. Evidence suggesting that the combination of these factors can significantly improve MH indicates the necessity of developing and implementing strategies that encourage regular PA and the strengthening of religiosity. These actions will not only help enhance the quality of life for OAs but also contribute to building a more holistic and effective healthcare model, guiding health professionals and researchers in creating tailored interventions for the well-being of this population.
Conclusion
Our study examined the interaction between resilience, PA, religiosity, and their influence on the MH of community-dwelling OAs. While our results indicated that religiosity and engaging in PA at least twice per week were associated with some MH benefits, the most pronounced effects were observed among those who engaged in PA three or more times per week. Moreover, high levels of resilience served as a protective factor for OAs who lacked regular PA and religiosity, contributing to better MH outcomes in these subgroups. These findings highlight the potential value of promoting resilience, regular PA, and religiosity as protective factors for enhancing MH in OAs. Further research in this area is essential to inform the development of integrated and multidimensional strategies for comprehensive MH care in aging populations.