Article Content
Introduction
CAMH is Challenging in Mainland China
Based on the statistics of the United Nations International Children’s Emergency Fund (UNICEF), approximately 1.3 billion teenagers fall into the age range of 10 and 19 constituting one-sixth of the world’s population (UNICEF, n.d.-a), with 14% of this cohort showing mental problems, accounting for a substantial 15% burden of disease in this demographic as of 2021 as the World Health Organization (WHO)’s statistics indicates (WHO, 2024). A meta-analysis of over 40 studies across 27 countries indicates that 6.5%, 5.7%, 3.4%, and 2.6% of adolescents showed symptoms of “anxiety disorders,” “disruptive disorders,” “attention deficit hyperactivity disorder (ADHD),” and “depressive disorders,” respectively (Polanczyk et al., 2015). However, children’s and adolescents’ mental health rights remain largely marginalized, particularly in low- and middle-income countries, where nearly 90% of them reside (WHO, n.d.-a).
In mainland China, the population aged 15 and below, encompassing children and adolescents, reached 239.08 million in 2022, which is 16.9% of the total population (National Bureau of Statistics of China, 2023), and studies have consistently indicated that psychological issues are prevalent. Notably, as early as the 1990s, a collaborative study by the WHO revealed a 7% prevalence of emotional and behavioral disorders among the 6–12-year-old student population in mainland China (Matsuura et al., 1993). A subsequent meta-analysis encompassing eighteen studies published between 1987 and 2011 reported a prevalence rate of 11.8 per 10,000 population for autism among children in China (Sun et al., 2013). Furthermore, in the first national-scale psychiatric epidemiological survey targeted at children and adolescents aged 6–16 years during 2014–2015 and issued in 2021, an overall prevalence rate of 17.5% for any psychiatric disorder was reported. Among the most prevalent psychological disorders in this population were “ADHD” (prevalence = 6.4%), “Oppositional Defiant Disorder” (prevalence = 3.6%), and “Major Depressive Disorder” (prevalence = 2%). Additionally, the survey demonstrated a higher incidence of psychological problems affecting children and teenagers residing in developed cities compared to those residing in less economically disadvantaged areas (Li et al., 2022a).
Moreover, evidence indicates that mental health problems in youngsters in mainland China have experienced an upward trend. Xin et al. (2012) reviewed four studies between 1992 and 2005 using an inter-temporal meta-analysis that demonstrated Chinese adolescents’ psychological well-being has declined across birth cohorts from the early 1990s onwards, with elevated anxiety symptoms and depression disorder, and a decline in self-esteem as a positive trait. Similarly, a three-round longitudinal survey using the “Mental Health Inventory of Middle School Students (MMHI-60)” found that adolescents surveyed between 2016 and 2020 had significantly increased levels of anxiety, emotional distress, academic stress, interpersonal sensitivity, obsessive–compulsive behaviors, and depression (Wu et al., 2022). A recent meta-analysis encompassing 191 studies during the COVID-19 pandemic involving more than one million underage students revealed the prevalence of anxiety, depressive symptoms, and sleep difficulties reached 31%, 31%, and 42%, respectively (Deng et al., 2023), these rates indicate an increase compared to the pre-pandemic period.
In summary, psychological challenges concerning children and adolescents in mainland China are not only pervasive but also display an upward trajectory. Extensive research consistently underscores that almost half of adult mental disorders arise and manifest for the first time during youth or earlier, before age 14 (Belfer & Saxena, 2006; Patel et al., 2007). Failure to address mental health issues during this critical developmental stage engenders enduring consequences that persist into adulthood and severely attenuate global well-being (Remschmidt & Belfer, 2005). Therefore, prioritizing Child and Adolescent Mental Health (CAMH) interventions has critical significance.
Sociocultural and Structural Context of CAMH in Mainland China
CAMH in mainland China is shaped by an interplay of sociocultural, economic, and policy-specific factors, posing unique contextualized challenges. Since China’s Reform and Opening-Up Policy in 1978, which catalyzed a shift toward a market-oriented economy and introduced Western values, particularly in urban regions, a hybrid cultural environment has been created with both traditional collectivist norms and globalization influences (Liu, 2003). Concerning it, two critical dimensions—urban–rural disparities and the examination-oriented education system—profoundly influence the design and implementation of mental health policies. First, China’s rapid urbanization has exacerbated inequalities in mental health service access, particularly for rural left-behind children (LBC). Studies show that LBC are more prone to suffer from mental health problems, such as anxiety and depression, compared with Non-LBC, compounded by fragmented familial support and limited access to mental health resources (Sun et al., 2021), with mental health professionals clustered in major cities in Eastern and Northeastern provinces, while limited in rural communities in Central and Western provinces (Sun et al., 2024). This urban–rural divide emphasizes the urgency of policies targeting equitable resource allocation, and the “National Mental Health Work Plan (2015–2020)” emphasizes grassroots service expansion (General Office of the State Council, 2015), but faces challenges in implementation due to workforce shortages.
Second, academic achievement, deeply rooted in Confucian values of endurance and diligence (Li, 2001), remains a cornerstone of familial and societal expectations. Mainland China’s education system shapes the school-based approaches to mental health policy. However, Gaokao (National College Entrance Examination) perpetuates intense academic competition, contributing to rising rates of stress, burnout, and suicidal ideation among adolescents (Fu, 2024). The PISA 2018 report highlighted that China scored significantly higher in reading than all other countries/economies and performed well in mathematics and science (OECD, 2019), while it comes at a cost of the cultural valorization of academic perseverance (Shek et al., 2013; Tan et al., 2025). Schools, often prioritizing performance over well-being, have been slow to adopt mental health interventions (Zhang, 2016).
Emerging policies, such as the “Double Reduction Policy” in 2021, exemplify efforts to reorient educational priorities toward student well-being, though challenges persist in ensuring schools relocate adequate resources to mental health-promoting activities (Jin & Zhang, 2022). The “Mental Health Action Plan for Children and Adolescents (2019–2022)” (National Health Commission of the PRC et al., 2019) signals a paradigm shift toward integrating CAMH into broader social and educational reforms. By situating CAMH within these dynamic socio-cultural and policy contexts, this study highlights the necessity of culturally informed, asset-based, and evidence-based approaches to support youth development.
CAMH Concept and Its Evolution
CAMH has increasingly evolved as a holistic construct that encompasses not only the absence of mental disorders but also the presence of cognitive, emotional, and social competencies. UN General Assembly (1989) emphasizes that mental health integrates developmental, educational, and social dimensions. Similarly, the WHO broadly defined mental health as “a state of well-being in which the individual realizes his or her own abilities, can cope with the normal stresses of life, can work productively and fruitfully, and is able to make a contribution to his or her community” (WHO, 2005, p. XVIII). Positive psychology (Seligman & Csikszentmihalyi, 2000) further validates the shift of conceptualizations from behavioral problems and diagnosable illnesses to a strengths-based framework that prioritizes positive youth development (PYD), early intervention, and ecological supports (Shum et al., 2025). Researchers identify CAMH as holistic psychosocial functioning and the dynamic capacity to achieve cognitive, emotional, and social development while maintaining adaptive resilience to stressors (Patel et al., 2008).
In mainland China, CAMH definitions have historically been defined from a narrow perspective, focusing on behavioral deviations and clinically defined mental illnesses (Kuo & Kavanagh, 1994). For instance, the purpose of the enactment of the “Mental Health Law of the People’s Republic of China” (issued in 2012, revised in 2018) is to safeguard the legitimate rights and interests of persons with mental disorders (National People’s Congress, 2012). However, with advances in cross-cultural health, policy discourse has increasingly incorporated holistic principles from international frameworks, such as the WHO’s “Healthy Life Course Approach” (Pan American Health Organization, 2020) and PYD models. For instance, the “Mental Health Action Plan for Children and Adolescents (2019–2022)” aims to promote the mental health and overall quality development of children and adolescents (National Health Commission of the PRC et al., 2019), thereby incorporating the treatment, prevention and developmental well-being across health, educational and social domains (Li et al., 2022b). In this study, CAMH is defined as beyond clinical well-being and encompassing positive developmental attributes, including the acquisition of age-appropriate cognitive, emotional, and social skills in harmony with sociocultural expectations such as collective responsibility.
Regarding the age range of CAMH, we define children and adolescents as individuals 18 years of age and younger, including kindergarten and primary to senior high school students, while excluding college students, aligning with international and domestic policy comparability, developmental science frameworks, and China’s legal and service systems. Firstly, international and domestic policy support defining childhood as extending until 18. While the National Bureau of Statistics of China (2002) classifies individuals aged 0–14 as juveniles and children for demographic reporting, China’s ratification of the “United Nations Convention on the Rights of the Child” (UNCRC) states that “child” refers to any person aged under 18 years (UN General Assembly, 1989), and the WHO (n.d.-b) defines “adolescence” as the period of life between childhood and maturity, spanning from ages 10 to 19. Domestically, the “Law of the People’s Republic of China on Protection of Minors” (issued in 1991, revised in 2024) states that “minors mean citizens under the age of 18” (Article 2) (National People’s Congress, 1991). Secondly, psychological developmental science demonstrates that pubertal development and psychosocial transitions remain salient until age 18 (Vijayakumar et al., 2018), and brain maturation, particularly in the prefrontal cortex and limbic system, persists into late adolescence (Crone & Dahl, 2012). Thirdly, pediatric services typically serve patients until age 18, after which transition to adult care begins (Castillo & Kitsos, 2017). Fourthly, sociocultural factors in mainland China reinforce the appropriateness of the 0–18 classification. China’s secondary education completion timeline (usually age 18) marks a crucial shift from familial supervision to independent living for college-bound youth, and physical separation and increased autonomy in decision-making would change mental health risk profiles (Fan et al., 2024; Yang et al., 2023). Besides, social expectations frame adolescence as a period of “preparation” for societal roles, extending protective oversight until emerging adulthood starting from age 18 (Fan et al., 2024). In summary, adopting the 0–18 range captures critical developmental junctures and aligns with both international frameworks and China’s legal and cultural contexts.
CAMH Policy as Government Commitment to Improving Mental Health
Numerous factors pose obstacles to the nourishment of CAMH, including limited financial and professional resources, difficulties in accessing psychological services, inadequate mental health education within schools, and societal misconceptions associating mental issues with stigma (Belfer, 2016). Among these factors, the absence of mental health policies tailored to youngsters stands out as particularly crucial (Belfer, 2016; Belfer & Saxena, 2006).
Public policy, as defined by Salisbury (1968), “consists in authoritative or sanctioned decisions by governmental actors. It refers to the ‘substance’ of what the government does and is to be distinguished from the processes by which decisions are made. Policy here means the outcomes or outputs of governmental processes” (p. 152). Consequently, CAMH policies serve as a guiding framework for government action (Shatkin et al., 2008), reflecting the government’s commitment and roadmap to address mental problems and enhance the well-being of young people as a collective. The policy outlines the goals, principles, vision, and values underlying mental health development. Its implementation has proven catalytic in increasing community interest in youth mental health, engaging stakeholders, ensuring oversight and accountability, mobilizing financial and resource support, and promptly addressing gaps in care.
Recognizing the crucial significance of policies concerning mental health, the WHO issued a recommendation in 1977 urging all countries worldwide to establish national plans covering mental health needs for children and adolescents. In line with this, the WHO released “The Mental Health Policy and Service Guidance Package: Child and Adolescent Mental Health Policies and Plans” in 2004, providing assistance to countries in developing CAMH policies. Furthermore, during “the 8th Global Conference on Health Promotion,” co-hosted by the WHO in 2013, the “Helsinki Statement on Health in All Policies” was endorsed. This statement prioritizes health and equity as fundamental responsibilities of governments towards their populations (WHO, 2014).
Moreover, the United Nations (UN) adopted the UNCRC in 1989, which outlines the fundamental right of children to receive mental health care. As of 2024, this convention has been endorsed by 197 economies (United Nations, n.d.). Additionally, The 2002 UN resolution on “A world fit for children: Resolution/adopted by the General Assembly” emphasizes the commitment to “care for every child: nurture children in a safe environment that enables them to be physically healthy, mentally alert, emotionally secure, socially competent and able to learn” (UN General Assembly, 2002, p. 2).
Many countries, particularly low-income and middle-income economies, often consider their ratification of the UNCRC as evidence of dedication to CAMH services. However, research indicates that mere endorsement of the UNCRC does not guarantee the construction of particular policies or program initiatives promoting the provision and support of mental health care for kids and youngsters (Belfer & Saxena, 2006). Therefore, there is a pressing need for a systematic policy review to address this gap.
The Fundamental Need for CAMH Policy Review
As highlighted by Shatkin and Belfer (2004), “no systematic study of the current status of international child and adolescent mental health policy exists” (p. 104). Recognizing this gap as well, the WHO took the “Atlas: Child and Adolescent Mental Health Resources” initiative in 2005 (updated in 2018 and 2021) to address the lack of comprehensive review and evaluation of CAMH policies at the global level (Belfer & Saxena, 2006; WHO, 2018, 2021). Notably, prior to the publication of the Atlas, there was no systematic research linking policy availability to identifiable planning initiatives.
Several policy reviews on CAMH have emerged in different countries and regions after the release of the Atlas. For instance, Kutcher et al. (2010) analyzed the availability and content of CAMH policies in all provinces in Canada, demonstrating that only four provinces have CAMH plans or policies, while the other provinces had no attempt to incorporate these elements into existing mental health strategies. Mokitimi et al. (2018) employed the Walt and Gilson policy triangle framework (1994) to search and identify all provincial CAMH policies across South Africa, showing that none of the provinces had a CAMH policy or plan to support the national CAMH policy, and CAMH professionals were not included in the policy development process, which aligns with concerning findings from other low- or middle-income countries, reinforcing the global neglect of CAMH at the policy level. While research interest in CAMH policy review has grown, systematic reviews of CAMH policies remain fundamentally deficient, particularly in developing countries.
The current lack of a systematic and critical review of CAMH policies in mainland China (Liang et al., 2017; Zhou et al., 2019) has left the Chinese government’s actual efforts, commitments, and effectiveness of the initiatives to improve CAMH largely unknown. This knowledge gap poses challenges in providing robust evidence and responding convincingly to the criticisms raised by various stakeholders. Furthermore, it hinders the identification of existing gaps and the implementation of timely remedies. By critically reviewing existing CAMH policies, this study acknowledges the efforts while identifying gaps, providing a reference for policymakers in making firm commitments and policy adjustments to nurture children and adolescents, as a vulnerable population with limited political representation or a “political voice” (Shatkin et al., 2008).
Methods
Epistemological Foundations of the Policy Review
Policy documents, as official records of government actions, provide a factual basis for analysis (Yang et al., 2020). Policy review examines the issuing body of the policy, its objectives, strategy scope, and implementation mechanisms, providing a qualitative, accessible, and cost-effective methodology (Stoffelen, 2019).
The study adopts a pragmatic, mixed-methods approach (Barnow et al., 2024; Brannen & Moss, 2012) to review CAMH policy in mainland China. Grounded in the pragmatic paradigm, which transcends rigid constructivist/realist binaries, we prioritize methodological pluralism and problem-solving utility over adherence to a single epistemological tradition (Patton, 2002). This stance aligns with contemporary shifts in evidence synthesis, where the “paradigms debate” has largely given way to a consensus among serious methodologists and practitioners for practical purposes on methodological flexibility and appropriateness (Bogna et al., 2020; Patton, 2002). As Patton (2002) argued, “A variety of methodological approaches are needed and credible … and that the challenge is appropriately matching methods to questions rather than adhering to some narrow methodological orthodoxy” (p. 264). Joint Committee on Standards for Educational Evaluation (1994) also reinforces this shift, advocating for methodological choices driven by research questions rather than paradigmatic orthodoxy. Demanding methodological purity risks oversimplifying the complexity and dynamic of real-world problems, which often demand adaptive, multidimensional approaches. Methodological openness, far from compromising validity, reflects the nuanced reality of knowledge creation (Bogna et al., 2020; Patton, 2002). By rejecting methodological tribalism, our pragmatic approach exemplifies the “end of the paradigms debate” (Patton, 2002, p. 264), providing a replicable model for policy review.
With respect to the mixed-methods approach, consistent with contemporary studies (Bogna et al., 2020; Patton, 2002; Shek, 2024; Tan et al., 2025), we employ “paradigm triangulation” (Barnow et al., 2024) of combining document analysis with social network analysis of the bibliometric method to balance interpretive depth with systematic pattern recognition. It is theoretically grounded in complementary strengths (Plano Clark, 2017) and is consistent with the trend of criticizing a single paradigm for its limitation, thus “strengthens the argument for marrying pluralistic theorizing to methodology, resulting in a research strategy based on paradigm triangulation” (Bogna et al., 2020, p. 465). While there are critiques of mixed methods, such as those by Guba and Lincoln (1988), caution against blending epistemologically incompatible approaches. However, as Patton (2002) argues, the practical imperative to address complex questions often outweighs concerns about paradigmatic purity. Human reasoning, in practice, is sufficiently nuanced to reconcile deductive hypothesis testing with inductive exploration.
Our policy review adopts a mixed-methods approach. We conducted a qualitative analysis of the themes derived from the existing policies, official figures, and scientific statistics, with semantic techniques employed to identify relevance to CAMH, the policy objectives, and target populations (Yang et al., 2020). Besides, to address the complexity of large-scale policy networks that traditional document analysis struggles with (Li et al., 2023; Yang et al., 2020), we employed social network analysis of the bibliometric method to reveal structural patterns (Donthu et al., 2021) (e.g., quantifying the dominance of the authority in policy networks), while qualitative analysis of examining available policy information enables us to interpret meaning-making in policy language, which contextualizes quantitative findings and exposes contradictions (e.g., interpreting the CAMH policy gaps). Our paradigm triangulation aligns with pragmatic methodology, where “what works” supersedes paradigmatic purity (Patton, 2002) to produce actionable policy implications.
Scoping Review Strategy
The scoping review is “a type of knowledge synthesis, follow a systematic approach to map evidence on a topic and identify main concepts, theories, sources, and knowledge gaps” (Tricco et al., 2018, p. 467), which applies to clinical guideline development and policy analysis. Policy texts were analyzed as dynamic artifacts shaping and shaped by sociocultural realities, consistent with the scoping review’s aims to “inform future research priorities, policy and on occasions influence practice” (Pollock et al., 2024, p. 5). Regarding the scoping review strategy, we follow and adapt the “Arksey and O’Malley framework” (Arksey & O’Malley, 2005) to ensure transparency and rigor, including six stages.
Stage 1: Identifying the Research Question
This policy review addresses two research questions.
- Research Question 1: What is the development of CAMH policies in mainland China?
- Research Question 2: What gaps exist in CAMH policies in mainland China?
Stage 2: Identifying Relevant Policies (Data Source)
The study reviewed policies at the national level, including laws, administrative regulations, legislation, guidelines, plans, programs, official opinions, circulars, and other normative documents. Data were sourced from three main databases: “The Chinese Central Government’s Official Web Portal” (http://www.gov.cn), “iPOLICY” (a database by Tsinghua University), and “PKULAW” (formerly LawinfoChina). Academic journals and online news reports were also included to ensure a comprehensive review. Search terms included “children,” “youth,” “students,” “primary and secondary school students,” “mental health,” “physical and mental health,” “moral education,” “school health services,” “CAMH Policy,” and “Health Policy.”
Data collection and analysis were conducted by four research assistants between April 2024 and July 2024, and the search covers policies issued since the establishment of the People’s Republic of China in 1949 (Table 1). To ensure accuracy and reliability, a rigorous protocol of repeated website visits was implemented for cross-checking and verification. A Research Assistant Professor (first author) reviewed the collected data, verifying key information, policy topic identification, and keyword summaries to minimize potential errors and inconsistencies.
Stage 3: Policy Selection (Inclusion Criteria & Screening Process)
According to three inclusion criteria of “CAMH Relevance” (i.e., related to CAMH), “National-Level” (i.e., excluded regional/local policies, and only include national-level policies), and “Active Status” (i.e., only include “in force” policies), 52 CAMH-relevant policies that were still in force were ultimately selected for analysis (Fig. 1).
- 1)Policy Theme Screening: Selecting topics explicitly targeting CAMH or implicitly addressing related themes.
- 2)Policy Level Screening: Focusing on national-level policies issued by the National People’s Congress and its Standing Committee, the State Council and relevant ministries and commissions, either individually or jointly.
- 3)Deletion of repealed policies: Including only policies that are still in force, excluding those that have been repealed.

Policy text screening flowchart
In addition, we adopted the following criteria to address revised and overlapping policies. For revised policies, only the latest revised version of a policy was included if stated as “in force.” For example, the “Mental Health Law of the People’s Republic of China” (issued in 2012, revised in 2018) was analyzed in its 2018 iteration; For coexisting Policies, if multiple versions of a policy were active, the latest revised version was included and analyzed.
Stage 4: Charting the Data
We employed a mixed-method policy review. Firstly, the thematic analysis focused on five dimensions and sub-codes in the “Thematic Coding Framework” (Fig. 2), including 1) “Policy Relevance”: to filter policies explicitly/implicitly addressing child and adolescent mental health; 2) “Target Population”: to categorize groups prioritized in policies; 3) “Policy Type”: to identify legal authority; 4) Issuing Authority: to map collaboration networks among policymakers; 5) “Policy Theme”: to classify policy content.
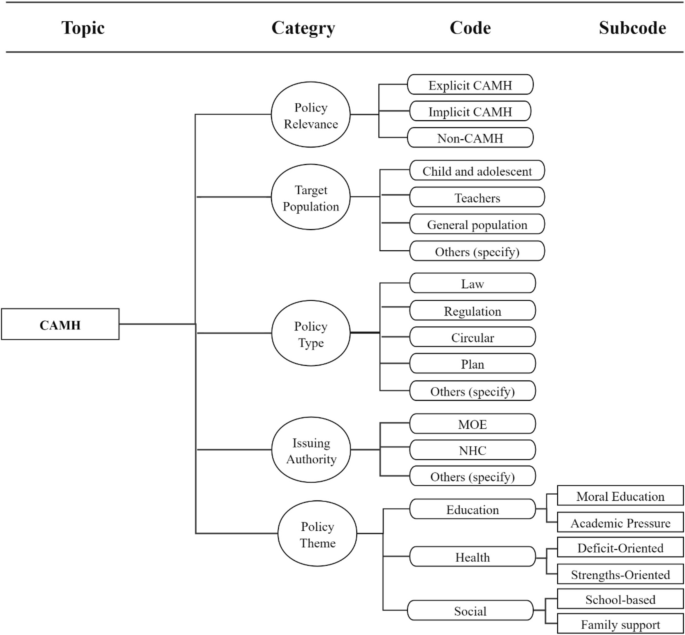
Thematic Coding Framework
Secondly, we employed Gephi 0.10.1, which is an open-source tool commonly used for real-time visualization of large networks (Bastian et al., 2009), for the social network analysis to map collaboration networks and identify key policymakers. The basic network statistics include “nodes” and “edges.” “Nodes” are the total number of organizations in the network, “edges” are the total number of collaborations (links) between organizations, and “edge weight” is defined as the frequency of collaboration between two agencies. Besides, the centrality measures, including “degree centrality” which is the number of direct collaborations an organization has, with high values that represent hubs of collaboration; “betweenness centrality,” which is the fraction of shortest paths passing through a node, with high values that act as bridges between disconnected groups; and “closeness centrality” reflects organizations with short paths to all others can disseminate policies efficiently. In terms of cluster structure, “modularity” measures the strength of division into clusters, with high modularity indicating distinct subgroups (Cherven, 2015).
Stage 5: Collating, Summarizing, and Reporting the Results
In this study, research results include findings of the collaboration network of CAMH policy issuing authorities and findings of policy content review, identified gaps, as well as policy implications proposed.
Results and Discussion
Trends in CAMH Policy Issuance
An upward trend in CAMH policy issuance was observed from 1991 to 2023 (Fig. 3), with sporadic policies in the early 1990s gradually increasing towards the late 1990s. The early 2000s showed gradual growth, intermittent rises, and a notable surge in the 2010s, peaking in 2015 and 2016. A substantial increase in policies was noted in 2021, despite a slight decline in 2022, followed by a resurgence in 2023. With respect to average annual growth rates and key motivating events. From 1991–2000, only 6 policies were issued (0.6/year), spurred by China’s ratification of the UNCRC in 1992, which catalyzed its earliest CAMH policies, such as the 1994 issuance of the “Opinions of the Central Committee of the Chinese Communist Party Regarding the Further Strengthening and Improvement of Moral Educational Work in Primary and Secondary Schools” (CPC Central Committee, 1994). However, growth remained slow, with sporadic issuance reflecting limited policy prioritization on CAMH. The 2001–2010 period had doubled output (12 policies, 1.2/year) with a growth rate of 100% compared to the 1990s, driven by the “686 Program” launched in 2004, also known as “The Community Management and Treatment Project for Severe Psychiatric Disorders,” as a national initiative to integrate mental health evaluation. Growth accelerated further in 2011–2020 (24 policies, 2.4/year) with a growth rate of 100% compared to the 2000s, following the 2012 “Mental Health Law of the People’s Republic of China” was enacted, which institutionalized CAMH priorities such as school-based interventions (National People’s Congress, 2012). The 2021–2023 period recorded the highest annual rate (3.3 policies/year, 10 total) with a growth rate of 38% compared to the 2010s, reflecting urgent COVID-19 responses (Shek, 2021). Overall, policy issuance escalated alongside major sociopolitical and public health milestones, while fluctuating growth rates underscore uneven development challenges over time.
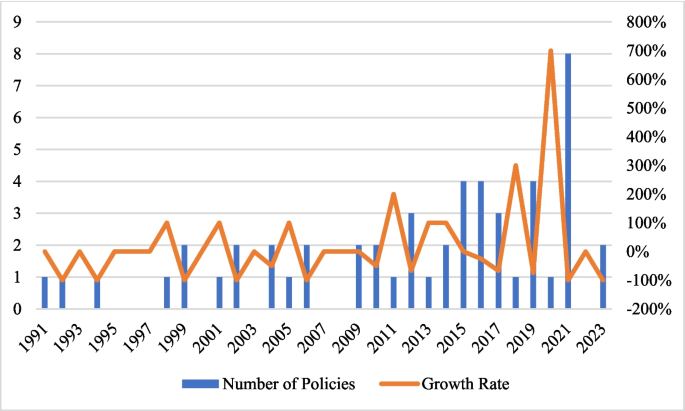
Number and growth rate of CAMH policies in mainland China
When compared to other countries, China’s trend in CAMH policy issuance aligns with global patterns of slow development, observed in both developed and developing economies. Shatkin and Belfer (2004) conducted an investigation collecting policy data from the WHO international databases and consulted psychiatrists worldwide. Their findings revealed that no country worldwide had developed mental health policies exclusively dedicated to children and adolescents, while only a mere 18% of the 191 member countries examined (35 countries in total) possessed mental health policies that had the potential to benefit this population to some extent. The WHO Child Atlas Project in 2005 further substantiated the lack of CAMH policies. Out of the 66 countries that responded to the survey, with no response from the remaining 126 member states, only 30 countries reported having national policies that encompassed children’s rights. However, these policies primarily concentrated on addressing cases of maltreatment, rather than encompassing the wider spectrum of mental health needs and PYD (Belfer & Saxena, 2006). In 2017, among the 78 countries that participated in the WHO Child Atlas Project survey, only 46% had established a CAMH plan or strategy (WHO, 2018). According to the recent 2020 WHO Child Atlas Project, 53% of the 168 respondents indicated the presence of dedicated psychological health plans or policies exclusively tailored for kids and teenagers with either stand-alone or integrated within existing frameworks (WHO, 2021).
In high-income economies such as the United States, Canada, the United Kingdom, and Europe, CAMH policies are relatively established (Zhou et al., 2020a), while they still face persistent challenges in forming a systematic CAMH strategy. The establishment of CAMH policy systems has followed nonlinear trajectories, often spanning decades of incremental reforms from an initial focus on care for severe mental disorders to advocating for school-based services, shifting from treatment to prevention. For instance, while national CAMH frameworks have been established, for example, the United Kingdom’s “Future in Mind (2015)” (Department of Health & NHS England, 2015) and Scotland’s “Mental Health Strategy 2017–2027” (Scottish Government, 2017) prioritize prevention and accessible services, Australia’s “National Children’s Mental Health and Wellbeing Strategy (2021)” integrates cross-sector collaboration and digital technology (National Mental Health Commission, 2021), these policies often struggle with inconsistent funding, workforce shortages, and fragmented service integration linked with decentralized systems (Kutcher & McLuckie, 2011). Similarly, Canada’s Evergreen Framework, which is the first national CAMH framework, though lauded for its emphasis on early intervention, faces criticism for uneven regional execution, overemphasis on clinical care, and a limited outcome evaluation (Kutcher & McLuckie, 2011). These highlight that even in developed countries, CAMH policies frequently lack robust linkages to actionable planning, monitoring, or equity-focused resource allocation. For developing economies, they face significant challenges in CAMH policy development. Several systematic reviews found that low- and middle-income countries not only lack CAMH policies but also encounter implementation challenges related to feasibility and sustainability, as the majority of them lack a dedicated budget for CAMH, and “out-of-pocket payments for services” are common. Such challenges are prevalent in economies such as South Africa, Ghana, India, Iraq, Uganda, Vietnam, and Zambia, as well as regions including Latin America, sub-Saharan Africa, and the Caribbean (Juengsiragulwit, 2015; Zhou et al., 2020a).
Collaboration Network of CAMH Policy Issuing Authorities
Figure 4 shows a network of interactions among entities involved in CAMH policy formulation. The node is 38 and the edge is 341, a network density of 0.485 shows moderate density, with nearly half of all possible edges present, suggesting moderately frequent collaborations between entities. The participation of various entities such as the “Ministry of Public Security” (MPS), the “All-China Women’s Federation” (ACWF), the “Ministry of Finance of the PRC” (MFO), the “National Development and Reform Commission” (NDRC), “State Administration of Press, Publication, Radio, Film and Television” (SAPPRFT), and the “China Association for Science and Technology” (CAST) indicating a broad collective effort to incorporate mental health factors into broader social and educational policies. However, the modularity analysis (Q = 0.159) suggests weak but detectable community division into four groups, reflecting overlapping policy interests rather than strict sectoral divisions.
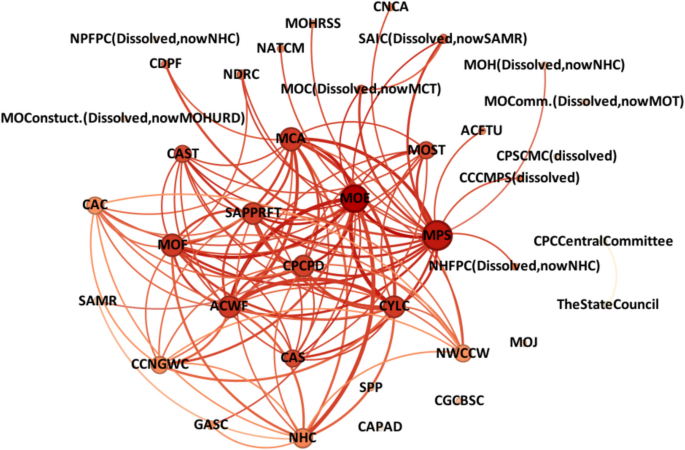
Collaboration network map of CAMH policy issuing authorities using Gephi 0.10.1 (Note. MOH = Ministry of Health; MCA = Ministry of Civil Affairs; MPS = Ministry of Public Security; CDPF = China Disabled Persons’ Federation; MOE = Ministry of Education; MOJ = Ministry of Justice; MOConstuct. = Ministry of Construction; MOHURD = Ministry of Housing and Urban–Rural Development; MOComm. = Ministry of Communications; MOT = Ministry of Transport of the PRC; SAIC = State Administration of Industry and Commerce; MOC = Ministry of Culture; MCT = Ministry of Culture and Tourism; CPCCentralCommittee = CPC Central Committee; TheStateCouncil = The State Council; ACWF = All-China Women’s Federation; CYLC = Communist Youth League of China; CCNGWC = China Cares for the Next Generation Working Committee; NHFPC = National Health and Family Planning Commission; NHC = National Health Commission; CPCPD = Publicity Department of the Communist Party of China; CCCMPS = Central Committee for Comprehensive Management of Public Security; NDRC = National Development and Reform Commission; MOST = Ministry of Science and Technology; MOF = Ministry of Finance of the PRC; MOHRSS = Ministry of Human Resources and Social Security; SAPPRFT = State Administration of Press, Publication, Radio, Film and Television; CAS = Chinese Academy of Sciences; NATCM = National Administration of Traditional Chinese Medicine; ACFTU = All-China Federation of Trade Unions; CAST = China Association for Science and Technology; CNCA = China National Committee on Ageing; CGCBSC = Central Guidance Commission on Building Spiritual Civilization; CAC = Cyberspace Administration of China; NWCCW = National Working Committee on Children and Women; GASC = General Administration of Sport of China; SPP = The Supreme People’s Procuratorate; CPSCMC = Central Public Security Comprehensive Management Commission; NPFPC = National Population and Family Planning Commission; CAPAD = China Association for Poverty Alleviation and Development; SAMR = State Administration for Market Regulation)
The network exhibits a short average path length (1.461), meaning nodes are closely connected with most pairs reachable within 1–2 steps, which indicates efficient policy dissemination but may also show over-reliance on central hubs. In terms of centrality metrics, “Ministry of Education” (MOE) emerges as the most central actor, with the highest node degree (35) and betweenness centrality (124.62), signifying its hub role as a critical broker and influencer in the formulation and dissemination of CAMH policies. This centrality is evidenced by its numerous connections with other key stakeholders, including the “National Health Commission” (NHC), the “Ministry of Civil Affairs” (MCA), the “Publicity Department of the Communist Party of China” (CPCPD); and the “Communist Youth League of China” (CYLC). Besides, MCA also exhibits high centrality (degree = 28), indicating its strategic positions. The “CPC Central Committee” (CPCCentralCommittee) and the “State Council” (TheStateCouncil) show maximal closeness centrality (1.0) shows direct access to other nodes, suggesting centralized decision-making bodies with shortest paths to all entities.
Edge weight analysis reveals intense collaboration frequency between CYLC and MOE, MOE targets NHC, ACWF targets CYLC, and ACWF targets MOE, with edge weights = 10, which are the thickest edges. The moderate ties exist in MCA-MPS (weight = 8), tied to civil affairs coordination, and weak ties (weights ≤ 3) involve agencies (e.g., CYLC-NDRC), demonstrating marginal roles in cooperation.
Policy Focus, Target Populations, Types, and Themes in CAMH Policies
Among the 52 CAMH-related policies analyzed, two categories were identified. The first category was “Explicit CAMH Focus,” which is directly CAMH-targeted policies (n = 7) with two criteria: 1) “Primary Recipients”: Children and/or adolescents are explicitly designated as the primary target population; 2) “Dedicated Mental Health Focus”: The policy’s core theme is exclusively centered on mental health, with dedicated provisions for CAMH. For example, the “Mental Health Action Plan for Children and Adolescents (2019–2022)” explicitly addresses CAMH through targeted interventions, fulfilling both criteria (National Health Commission of the PRC et al., 2019).
The second category is “Implicit CAMH Focus,” which is indirectly relevant policy but with CAMH components (n = 45). These policies fall into two conditions: 1) Secondary CAMH components in non-child and adolescent targeted population policies: Policies that primarily target other populations (e.g., teachers, the general public) but contain secondary provisions and items concerning CAMH. For instance, “Opinions of the Ministry of Education on Strengthening the Training of Primary and Secondary School Teachers” focuses on teacher training while integrating student mental health support modules (Ministry of Education, 2011); 2) Indirect CAMH relevance in child and adolescent-targeted policies: Policies addressing children and/or adolescent populations but not primarily focused on mental health. For instance, the “Law of the People’s Republic of China on Protection of Minors” (issued in 1991, revised 2024) emphasizes safeguarding minors’ legal rights (e.g., personal and property rights) but includes provisions relevant to psychological well-being within protective frameworks (National People’s Congress, 1991).
Concerning the target population, the 7 explicitly CAMH-focused policies targeted primary/secondary students (n = 5), and children/teens (n = 2); while 45 implicit policies addressed the general public (n = 14), teachers (n = 2), children/minors/adolescents (n = 12), and kindergarteners/primary/secondary/general students (n = 17). In summary, among the 52 analyzed policies, 36 policies target children and adolescents, with varied expressions such as children, minors, primary and secondary students, and kindergarten students, 14 policies target the general public, and 2 policies address teachers (Table 2).
Regarding policy types, only four of the 52 policies are laws. These include the “Law of the People’s Republic of China on Protection of Minors” (issued in 1991, revised 2024) (National People’s Congress, 1991), the “Law of the People’s Republic of China on Prevention of Juvenile Delinquency” (issued in 1999, revised 2020) (National People’s Congress, 1999), the “Mental Health Law of the People’s Republic of China” (issued in 2012, revised 2018) (National People’s Congress, 2012), and the “Law of the People’s Republic of China on Family Education Promotion” (2021) (National People’s Congress, 2021). Notably, none of these laws are exclusive to CAMH, although they address related issues. The remaining documents consist of departmental regulations and other normative documents, such as official opinions, outlines, plans, and circulars.
In terms of policy themes, only seven policies exclusively address the mental health of children and adolescents. These include “Opinions of the Ministry of Education Regarding the Strengthening of Mental Health Education in Primary and Secondary Schools” issued by the MOE in 1998 (Ministry of Education, 1998); “Guidelines for Mental Health Education in Primary and Secondary Schools, Ministry of Education” by MOE in 2002 (Ministry of Education, 2002) and last revised in 2012; “Circular of the Ministry of Education on the Implementation of the Programme for the Creation of Schools with Characteristics in Mental Health Education in Primary and Secondary Schools” issued by MOE in 2014 (Ministry of Education, 2014); “Mental Health Action Plan for Children and Adolescents (2019–2022)” jointly issued by 12 authorities in 2019 (National Health Commission of the PRC et al., 2019); and “Circular of the Ministry of Education on Strengthening the Management of Students’ Mental Health” issued in 2021 by MOE (Ministry of Education, 2021a), among others.