Article Content
Abstract
Individuals affected by chronic fatigue often experience unpredictable fluctuations in their symptoms and activity levels, often leading to a perceived loss of control. This paper presents an explanatory model for understanding coping behaviors in chronic fatigue from the perspective of Cognitive Behavioral Therapy. As a comprehensive framework for patients and therapists, we introduce the Model of Active and Protective Coping for Chronic Fatigue (APC-Model), integrating clinical observations, existing knowledge, and the principles of behavioral analysis. The model identifies two dysfunctional behavioral patterns: Active Coping, by which individuals overexert themselves, and Protective Coping, by which activity levels become too low. Patients may alternate between these patterns, thereby exacerbating symptoms. The APC-Model suggests stabilizing activity levels within the individual’s area of endurable load as a major goal to enhance symptom management and control. Applying behavioral analysis separately to each dysfunctional coping pattern can help patients detect and disentangle the underlying and the maintaining factors, as well as those contributing to the shift between coping patterns. We illustrate with a case study suffering from chronic fatigue as part of post COVID, how this approach provides a valuable tool for deriving points of intervention and treatment strategies for individuals affected by chronic fatigue. We provide therapeutic material to support its practical application in English and German.
Explore related subjects
Discover the latest articles and news from researchers in related subjects, suggested using machine learning.
- Behaviorial Therapy
- Cognitive Behavioral Therapy
- Person-Centered Psychotherapy
- Systems or Family Therapy
- Therapeutic Relationship
- Adaptive clinical trial
Introduction
Chronic fatigue affects 10.1% of the adult population (Yoon et al., 2023), is associated with various diseases, and significantly impacts quality of life (Park et al., 2024). Individuals with chronic fatigue encounter a severe lack of energy and tiredness most of the time, which can make daily activities like taking a shower, or going to work or school, difficult. They experience multifaceted symptoms, which can vary widely both inter- and intra-individually. Often impaired cognitive and physical functioning are involved and may additionally be accompanied by affective symptoms. Individuals with chronic fatigue face the challenge of adapting their lives to a reduction of endurable load (Davis et al., 2023; Koczulla et al., 2024).
A key problem is that chronic fatigue frequently goes along with unpredictable fluctuations in quality and intensity of fatigue symptoms, often as part of post-exertional malaise (PEM). PEM refers to a worsening of symptoms following even mild activities, starting with a delay of several hours and lasting up to several days (Holtzman et al., 2019). The vague nature of fatigue symptoms makes it difficult to establish a clear understanding of the individual threshold of endurable load. This lack of predictability and perceived lack of influence on the symptoms contributes to a sense of losing control. Consequently, it hampers the ability to actively plan one’s life and results in heightened levels of distress (Bierbauer et al., 2022; Wurz et al., 2022).
When addressing chronic fatigue symptoms during psychotherapy, pacing principles often are incorporated. This entails encouraging patients to engage in activities to the fullest extent possible while respecting the constraints posed by their illness (Goudsmit et al., 2012). Programs using this approach specifically share a common objective regarding the patients’ activity levels: preventing overload while simultaneously avoiding dysfunctional protective behavior (e.g., Hasting et al., 2023; Sachenbacher et al., 2023; Schilling et al., 2023). This is a difficult act of balancing. Some authors describe that individuals affected by chronic fatigue often show notably and problematic fluctuating activity disregarding their thresholds of endurable load, a pattern often referred to as “all-or-nothing”, or “boom and bust” behavior (Gaber, 2021; Köllner et al., 2022).
Chronic fatigue also is the symptom contributing the most to functional impairment among patients with Post COVID-19 condition (short: post COVID; Walker et al., 2023). Post COVID is a chronic health condition with symptoms that appear at least three months after an acute infection with SARS-CoV-2, lasting for more than two months (ICD-10, U09.9). Based on a German population, the overall estimate for post COVID ranged from 6.5 to 28.5% in the infected adult population (Peter et al., 2022). The growing number of individuals experiencing this condition underscores the urgent need for a better understanding of chronic fatigue and the development of novel interventions.
In this paper, we propose a novel framework for psychotherapy, including an explanatory model and intervention tool that allows for an individualized approach tailored to patients with chronic fatigue, presenting fluctuating symptoms and activity levels. The central element is the Model of Active and Protective Coping for Chronic Fatigue (short: APC-Model), which clusters patterns of dysfunctional behavior into phases of Active and Protective Coping. The model offers both patients and therapists a shared framework for working towards understanding underlying mechanisms of fluctuating dysfunctional behavioral patterns and deriving adaptive strategies to stay within the individual’s “green area” of endurable load. To identify the initiating, contributing, and maintaining factors for both Active and Protective Coping phases, principles of behavioral analysis are applied.
Based on a case study with post COVID and moderate chronic fatigue, we illustrate the application of our APC-Model and illustrate how the identified factors can then be addressed to stabilize activity levels, improve coping with fatigue symptoms, and increase well-being. To support its practical application, we provide therapeutic material in Online Resource 1.
Framework: Model of Active and Protective Coping (APC-Model)
Key elements of the Model of Active and Protective Coping for Chronic Fatigue (APC-Model) are a reduced threshold of endurable load and patients’ activity fluctuating around this threshold, being categorized into Active and Protective Coping (see Fig. 1).
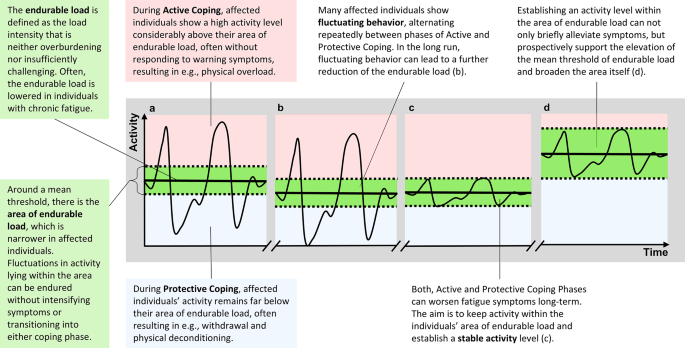
Visualization of the model of active and protective coping for chronic fatigue. Note. The line reflects an individual’s activity level (y-axis) over a period of time (x-axis). The green area between the dotted lines indicates the area of endurable load with a mean threshold of endurable load (bold line). Activity within the red section above the upper bound of the endurable load area lies within Active Coping. The blue section underneath the lower bound indicates Protective Coping. (a): Individuals show activity levels repeatedly fluctuating between Active and Protective Coping, leading to (b) a further decrease of the endurable load. After (c) a stable activity level within the area of endurable load, over time, chances increase for (d) an elevated mean threshold and a broadened area of endurable load
Area of Endurable Load
In the APC-Model, the endurable load is defined as the load intensity that neither overburdens nor insufficiently challenges the patient. According to the APC-Model, there is an area of endurable load around a mean threshold (displayed as “green area” in Fig. 1). Activity levels within the area are considered to be endured by individuals without intensifying fatigue symptoms or transitioning into adverse Active or Protective Coping patterns. We assume that (1) the mean threshold is lower in patients affected by chronic fatigue than before their illness, and (2) that the area of endurable load around the threshold is narrower.
The precise factors causing this reduction remain not fully understood. We advocate for the adoption of a comprehensive bio-psycho-social framework (Engel, 1977). Significant evidence indicates that biological factors, such as inflammatory and autoimmune processes, play an important role in chronic fatigue symptomatology, particularly when associated with post COVID (Al-Aly et al., 2024). At the same time, especially with respect to persistence, psychological and social factors are expected to contribute substantially (Lemogne et al., 2023). Regardless of which factors are responsible for the decline of endurable load, the APC-Model serves as a supportive tool to establish a balanced activity level in accordance with the individual’s capacities.
Activity: Active and Protective Coping
At the core of our Model of Active and Protective Coping (APC-Model), there is the individuals’ activity level, often fluctuating. We define activity broadly, including physical tasks (e.g., forms of movement, chores), cognitive demands (e.g., reading, or office work), and consider emotional load as equally important. Emotional load can include adapting to new capacities and roles, workplace conflicts, financial concerns, or challenging conversations, e.g., justifying oneself in personal and professional settings. Importantly, activity also includes desired aspects, e.g., the pursuit of the fulfillment of psychological needs like social connection.
We define two activity patterns: Active and Protective Coping. The two distinct dysfunctional patterns can manifest themselves across different levels of experience and behavior, including motor-behavioral, cognitive, emotional, and physiological levels. In Active Coping, patients show a high activity level considerably above their individual area of endurable load without responding to warning symptoms. This results in an overload and a performance drop. In contrast, during Protective Coping, patients’ activity remains far below their area of endurable load, resulting in e.g., withdrawal and physical deconditioning. As two contrasting approaches, phases of Active and Protective Coping can alternate repeatedly.
In line with Pacing principles (Goudsmit et al., 2012), our model aims to establish a stable activity level within the individuals’ area of endurable load. During Active Coping, reducing activity to a reasonable level may allow stress systems to recover, thereby alleviating symptoms and increasing stress tolerance over time (Jason et al., 2009). Similarly, increasing activity from Protective Coping will expose the patient to a higher still endurable activity level that opens the potential for a training effect. A reasonable level of activity adapted to the individual’s capacities may, for example, improve the chance for more stability in participation in social and professional life, which may stabilize experiencing positive reinforcements and a sense of self-efficacy. We hypothesize that establishing an activity level within the area of endurable load can not only briefly alleviate symptoms, but prospectively has the potential to support the elevation of the mean threshold of endurable load and broaden the area itself (see Fig. 1 (d)).
By use of our study case, we will illustrate how the previously described Model of Active and Protective Coping (APC-Model) and principles of behavioral analysis can be applied in the therapeutic process.
Treatment Implementation Illustrated by a Case Study
Case Study: Background Information and Description of the Presenting Problem
The presented case-study is a woman in her mid-forties with a reduced threshold of endurable load since her first SARS-CoV-2 infection, about a year before beginning psychotherapy. She was diagnosed with post COVID-19 condition, unspecified (U09.9), adjustment disorder with anxiety (F43.22), and other specified mental disorders due to known physiological conditions (F06.8), based on ICD-10. She attended 24 primarily weekly sessions of individual Cognitive Behavioral Therapy. The patient had been employed full-time in an administrative role until her SARS-CoV-2 infection. One year later, at the start of therapy, she was undergoing vocational reintegration, working 1–2 h daily. She reported cognitive deficits in concentration and memory alongside a mood marked by worry, despair, and sadness. She expressed feelings of helplessness and fear of losing autonomy, worthlessness, self-doubt, and excessive rumination, as well as exhaustion ranging from weakness to complete depletion. Physically, she described headaches, a burning, itching sensation on her scalp, an increased need for rest and sleep, rapid sensory overload, and noise intolerance.
Clarification of Objectives
At the beginning of treatment, therapeutic objectives should be clarified early on to prevent false expectations. It should be communicated that the first aim is to achieve stable activity levels and prevent symptoms from further deteriorating (see also Gaber, 2021) by staying within the area of endurable load. The chance to gradually increase the threshold of endurable load, however, may arise in the long term.
Introduction of the APC-Model as Common Therapeutic Framework
After clarifying the objectives, the Model of Active and Protective Coping for Chronic Fatigue (APC-Model) can be introduced as a common therapeutic framework to keep track of both dysfunctional and functional behavior and phasic shifts. An important goal of psychoeducation is to convey a clear understanding that activity levels significantly higher and lower than the endurable load may risk worsening symptoms. Therefore, activities should require load within the area of endurable load. As one goal of treatment, this concept focuses on the management of behavior instead of symptoms in order to strengthen a person’s perceived self-efficacy and sense of control.
Conceptualizing Behavioral Patterns: Applying Behavioral Analysis
Given the interindividual heterogeneity of symptoms, we argue that it is essential to identify individual factors that contribute to the dysfunctional behavioral patterns. In the following, we focus on a deeper understanding of specific behavioral patterns within Active and Protective Coping and on analyzing them to derive targeted therapeutic implications.
As an established framework for behavioral analysis, the SORCK model developed by Kanfer et al. (2012) is a supportive tool to explain and derive therapeutic interventions for problematic behaviors linked to complex syndromes. It explains behavioral (problematic) responses (R) in specific situations (S) along with their consequences (C) and contingency (K), while, within the organism variable (O), considering relatively stable bio-psycho-social factors that influence an individual’s spectrum of behavioral patterns. Since we identified Active and Protective Coping as the two major behavioral patterns between which chronic fatigue patients characteristically shift repeatedly (see Fig. 1), it is central to our model to work with two distinct conceptualizations —one for each coping pattern. By adapting SORCK principles, the therapeutic process now focuses on understanding the dynamics of emotion, cognition, and behavior for both phases, aiming to identify individual factors that drive and maintain patients in the Active and, respectively, Protective Coping phase (as depicted in Fig. 2). This said, these analyses can also lead to revealing situations with functional behavior, which then should be reinforced. Ultimately, these insights guide deriving and implementing interventions that provide the patient with adaptive strategies to keep activities within the endurable load.
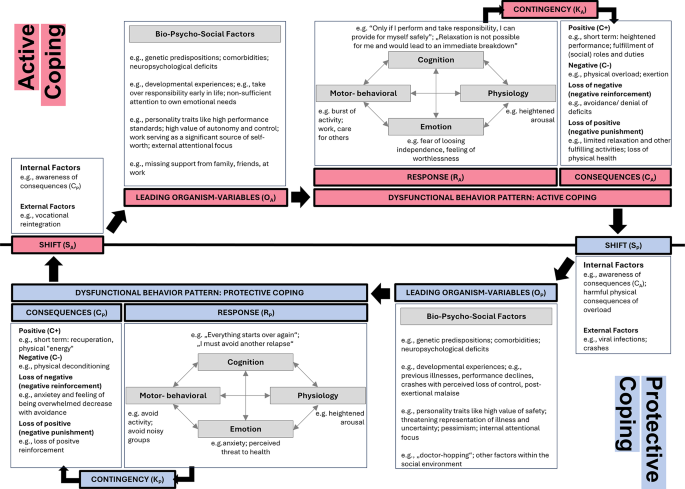
Application of an adapted version of the SORCK-model to active and protective coping
Conceptualization of Active Coping
Organism-Variable (OA)
On the biological level, the patient reports neuropsychological deficits in memory and executive functions. Psychosocially, she has high performance standards, as measured by the Young Schema Questionnaire (YSQ; Young, 2005). Work is a significant source of her self-worth, and autonomy and control are crucial psychological needs (Grawe, 2004) to her, as indicated by the Questionnaire for the Analysis of Motivational Schemas (FAMOS; Holtforth & Grawe, 2000).
We argue that when vulnerable aspects of the organism variable (OA) are triggered or become the patients’ focus, they respond to daily life situations and challenges with dysfunctional behavioral patterns. Our patient’s aversive representation of low performance is amplified by the unmet need for autonomy and control as a consequence of her illness. To compensate, she responds with Active Coping behavior, which manifests in motor-behavioral, cognitive, emotional, and physiological levels as indicated by the response variable.
Response-Variable (RA)
Active Coping is characterized by a burst of activity on a motor-behavioral level, such as working, sports, leisure, or caring for others. In our study case, this pattern is linked to cognitions like “Only if I perform and take responsibility, I can provide for myself safely” and “Relaxation is not possible for me and would lead to an immediate breakdown.” These cognitions are highly threatening to her due to their strong link with her aversive perception of low performance. She responds with fear of losing independence and feelings of worthlessness and with a diffuse sense of inner restlessness and heightened physiological arousal.
Consequences (CA)
In the short-term, Active Coping allows the patient to momentarily show a heightened performance and fulfill her (work/social) roles and duties (positive reinforcement; C+). Her high activity level is negatively reinforced as it helps to temporarily avoid confronting her deficits and fear of losing autonomy and control (C-/). Shaped by her biography, this compensating behavior with the underlying motives was likely effective before post COVID. However, with reduced energy, maintaining high activity levels is associated with physical and psychological overload and a further performance decline (C-). As symptoms of overload, our case reported, for example, heightened sensitivity to noise, headaches, and prolonged sleep (> 11 h per night plus sleep around lunchtime).
Derived Points of Intervention and Treatment Strategies for Active Coping
Applying the Model of Active and Protective Coping (APC-Model) and behavioral analysis resulted in two separate case conceptualizations, one for each coping phase. For Active Coping, we identified the following major points of intervention: (1) perceived neuropsychological deficits, (2) lowered self-worth, (3) high activity level leading to overexertion, (4) avoiding confrontation with deficits, and (5) perceived loss of autonomy and control. Once the points of intervention are derived from the conceptualizations, the therapist can use established treatment strategies for the respective points. In the following, we elaborate on possible therapeutic strategies by use of examples from our study case.
(1) Addressing perceived neuropsychological deficits: The reported deficits in memory and executive functions can be addressed with established neuropsychological training strategies while ensuring that the training remains within the area of endurable load. However, for our case mainly compensatory strategies with a focus on energy management were implemented. The patient’s priority was to establish a stable performance during reduced working hours. Time with more intense cognitive activity was therefore purposefully saved for work.
(2) Addressing reduced self-worth based on performance and external evaluation: The patient’s attention was directed towards sources of self-worth beyond work achievements or external judgment and towards realizing small steps in the process.
(3) Phases of overexertion: We hypothesize that during Active Coping, the individual’s attentional focus is external, lying on performance, financial consequences, and/or the evaluation of the social environment while ignoring internal symptoms, such as emotions, early signs of fatigue like bodily symptoms of overexertion. Awareness of these symptoms were improved through regular mindfulness exercises and a fatigue diary, considering emotional, physical, and cognitive aspects. To prevent overexertion and crashes, the therapeutic process included empowering the patient to set healthy boundaries, and teaching pacing strategies like incorporating regular and mindful breaks within her (work) day structure.
(4) Careful confrontation with deficits: The study case was gently confronted with her current deficits and the unforeseeable course of her illness, validating emerging emotions such as mourning the loss of her former self. This process was supported by elements from Acceptance and Commitment Therapy (ACT).
(5) Addressing perceived loss of autonomy und control: Through psychoeducation, we helped her understand the mechanisms behind her symptoms, thereby restoring a sense of control. This includes redefining autonomy and control considering her current capabilities. By applying an adapted fatigue diary (see Online Resource 2), and weekly assessing and categorizing her behavior into Active and Protective Coping phases, she was able to establish a link between activities and symptoms, enhancing her sense of control and self-efficacy.
Conceptualization of Protective Coping
Organism-Variable (OP)
Protective Coping (OP) as a response may come particularly at play, when on a biological level the patients have experienced harmful consequences of overload. These include intense fatigue symptoms and muscle pain, often referred to as “crashes,” especially in the context of Post-Exertional Malaise (PEM). Relevant developmental experiences of our study case include severe impairment after an Epstein-Barr virus infection approximately 25 years earlier, causing significant career changes. During phases of Protective Coping, her tendency towards pessimism may be amplified, as indicated by the Young Schema Questionnaire (YSQ; Young, 2005). Other traits triggering Protective Coping include a high need for safety and control and low risk-taking tendencies. The attentional focus shifts to internal factors like bodily symptoms.
Response-Variable (RP)
We again argue that when critical aspects of the organism variable (OP) are pronounced or activated, patients may respond to daily life situations and other challenges (see, e.g., Shifts SP) with Protective Coping strategies that reach dysfunctional levels. In our study case, Protective Coping occurred when being overly anxious about a relapse. Her behavior was characterized by avoidance of activities, e.g. avoiding noisy crowds or any work and social interactions. This behavior was accompanied by cognitions such as “I must avoid another relapse”, and “I may need my energy for something more relevant”, which are strongly associated with previously experienced crashes. On a physiological level, the individual exhibited signs of high physiological arousal, such as increased heart rate and muscle tension, reflecting a bodily response to perceived threats and stressors. The arising emotions included anxiety, a sense of threat to health, and a fear of losing control over her own body.
Consequences (CP)
As a short-term consequence of the Protective Coping response pattern, individuals are able to recover physically from overload (negative reinforcement; C-/) and experience relaxation (positive reinforcement; C+). However, in the long term, a dysfunctional low level of activity is associated with physical deconditioning (C-). Additionally, by withdrawing from professional and social roles (e.g., beloved creative tasks, coffee breaks, family dinners), the patient lost significant sources of self-worth and endangered the fulfillment of her need for attachment (C+/).
Derived Points of Intervention and Treatment Strategies for Protective Coping
While mainly showing a tendency towards Active Coping, our study case shifted into Protective Coping behaviors after viral infections. We identified the narrow focus on fear of symptom deterioration and the responded withdrawal as major points of intervention during Protective Coping.
Treatment strategies involved (1) validating the triggered fears of massively worsening symptoms and explaining them within the context of the previously mentioned developmental factors. At the same time, we (2) gently educated her about the relationship of monitoring body symptoms too closely and thereby reinforcing them (Bushnell et al., 2013). We also elaborated that withdrawing from rewarding activities more than necessary can cause her to remain below her potential for antidepressant behavior and risk further deconditioning of her body. We helped her (3) broaden her attentional scope from a narrow focus on fear of symptom deterioration to more external stimuli, such as other unmet basic needs, e.g., attachment. We identified her values and needs (i.e., based on Grawe’s concepts; Grawe, 2004) and (4) derived and planned activities to meet them within her potential and limitations.
Phasic Shifts (SA and SP)
Since patients experience unexplained fluctuations in their behavior, we consider it essential to identify typical situations that precede a shift to Active or Protective Coping. We assume that these turning points can be triggered by internal or external factors. Internal factors may involve realizing the consequences of the preceding coping pattern. A shift to Protective Coping can be preceded by realizing that excessive Active Coping went along with intensified fatigue symptoms. External factors can include job-related pressure or financial concerns, triggering a shift from Protective to Active Coping. We recommend collecting typical factors and derive and practice specified functional strategies with the patient that he or she can apply instead of re-engaging in dysfunctional behavioral patterns.
Balancing Active and Protective Coping Behavior To Stabilize Activity
When contrasting and regulating Active and Protective Coping behaviors, certain needs or experiences may seem contradictory and difficult to reconcile, appearing to exclude one another like opposing poles. This reflects the inner conflict many individuals face being torn between which needs to prioritize, possibly explaining the observed “all-or-nothing” behavior. According to our model, during any phase of dysfunctional coping, the focus tends to be heavily on one pole of needs, while the other is neglected. For example, our patient focused on reducing activities to avoid health setbacks, thereby neglecting social needs or needs for pleasure (Grawe, 2004). The metaphors of a pendulum vs. a scale can be helpful here, representing the back-and-forth movement vs. balancing between perceived opposing needs. The therapeutic challenge, then, is enabling the patient to acknowledge and integrate both sides within their potential, increasing flexibility towards adaptive behavior. Based on our study case, we will illustrate the conflict between seemingly opposing needs and the therapeutic approach to help her find a balanced solution. For another example, see Online Resource 3.
Our patient has been applying pacing strategies to manage her fatigue symptoms for the past couple of months. She had reduced the pleasurable activities that formerly had been part of her daily routine. She paid attention to receiving enough sleep and breaks, not extending her planned working hours. This led to a change in work content. She eliminated the more exciting and creative tasks and concentrated on administrative tasks that were rather boring but necessary for the job. After several weeks, she reported feeling better and a slight increase in energy levels, also reflected by slowly increasing her working hours. Now she received the opportunity to engage in an additional creative project, which had to take place during the night. However, she faced an internal conflict: wanting to reward herself with more exciting tasks at work (need for pleasure) but fearing overexertion and another setback (need for control over health). She is deeply caught in this conflict and feels pressured to make an all-or-nothing decision as if she must choose one side over the other. The described inner conflict arises from two opposing motives:
- Active Coping: “I deserve to treat myself this week. I want to finally enjoy work again.” This reflects her need for pleasure, which she feels entitled to fulfill, especially after sacrificing it for so long.
- Protective Coping: “I need to hold back—it would be better for my health [and ability to work] to withdraw. I can’t afford another crash.” This reflects her need for control over her health and needs for self-esteem protection and independence through performance at work.
Guided during the therapeutic process, she was able to reflect on overwhelming aspects of the creative task, including staying up late and being filled with excitement. She anticipated a crash that she only could counteract by extended rest. These insights allowed her to consider restructuring and reducing her working hours for the week to be able to get the rest needed to compensate for this extra task at night – a solution that she earlier would not have considered. In the next session, she reported that she had felt more fatigued for two days, but that she was able to manage the significantly reduced timetable without ending in a crash. She highlighted the joyful moment of creativity and mentioned that her mood had profited significantly from this endeavor. This observation indicates that her balanced approach considering differential needs had a positive impact on her emotional well-being without sacrificing physical health.
Outcome
The therapeutic process aimed to provide stabilizing support during the patient’s vocational reintegration. By the end of therapy, the following goals were achieved: stabilizing activity at an appropriate level, and improving coping with performance declines.
Details on the diagnostic assessment are provided in Online Resource 2. Pre and post treatment, the COGBAT (Aschenbrenner et al., 2012)—a computerized test battery for neuropsychological assessment—was conducted to evaluate attention and executive functions. The results indicated average cognitive performance both before and after therapy, with no clinically relevant changes observed over the course of treatment.
However, she developed a sustainable energy management and improved her ability to cope with fatigue. Over the course of therapy, both the clinical impression and the patient’s self-assessment regarding cognitive performance, resilience, mood, and anxiety improved. These impressions drew upon enhancements in both private and professional life, with her daily working hours gradually increasing from two to five hours alongside an expansion of private activities. This progress was also reflected in a reduction in depressive symptoms from moderate (BDI-II score = 15) to minimal severity (BDI-II score = 9; Beck Depression Inventory II, Beck et al., 2009). As a result, the initial diagnoses of F06.8 and F43.22 could be considered largely remitted by the end of therapy. Possibly associated with the described increase in activity, self-reported severe fatigue symptoms (Fatigue Scale for Motor and Cognitive Functions, Penner et al., 2009) showed only minimal improvements (FSMCpre = 82; FSMCpost = 74).
Discussion
In this paper, we introduced a therapeutic framework designed for chronic fatigue patients and illustrated its application in the context of post COVID. This framework, the Model of Active and Protective Coping for Chronic Fatigue (APC-Model), integrates clinical impressions from neuropsychological psychotherapy, insights from the current literature, and established principles of Cognitive Behavioral Therapy.
A key innovation of this model is its ability to dynamically reflect the fluctuating nature of both fatigue symptoms and activity levels by characterizing two major coping patterns—Active and Protective Coping—and illustrating their interplay. This new perspective offers therapists a comprehensive approach to consider both coping styles and phases. The underlying needs are considered, which are often perceived as conflicting by the patients themselves. For example, patients’ needs for activation and rest are disentangled and addressed within a single cohesive framework. Additionally, the model dynamically illustrates shifts between coping phases, helping therapists and patients alike to better understand and respond to these changing patterns. This structured approach enhances formulating interventions that are specific to each phase and individual, supporting both therapeutic planning and the patient’s perceived sense of control. Our clinical experience shows that the APC-Model for Chronic Fatigue is easily comprehensible for patients and provides a visual and tangible understanding of their condition. It serves as a guiding tool throughout therapy, offering a common language and memorable visual representations. Therapy materials and visual aids are included in Online Resource 1 to support its practical application.
Despite its potential benefits, there are some limitations to our model. The recommendations for its practical implementation are mainly based on clinical experience, and its applicability and effectiveness require empirical validation. The systematic empirical validation should include a suitable and comprehensive set of measures to assess symptom development across all dimensions of fatigue, extending beyond those available in our case study. One challenge within the implementation of our model is the complexity of fatigue symptoms and associated behavior. Part of this complexity is the interaction and overlap of various post-COVID (or other disease-related) symptoms. Addressing this requires an interdisciplinary approach. Our model adds to the psychotherapy-perspective and is complemented by others, such as pulmonary diagnostics and advice on the planning of physical activity. Within behavioral analysis, these aspects (e.g., diagnosed pulmonary impairments) can be included into our model within the Organism-Variable. However, such interdisciplinary collaboration demands significant resources from both caregivers and patients (Hayden, 2024).
Another barrier to its implementation is patient skepticism towards psychotherapy, often driven by stigma around psychological treatment and fears of not being taken seriously. These concerns are reinforced by a misleading dualistic separation of psychological and biological mechanisms, particularly in the context of post COVID (Lemogne et al., 2023). To counteract this, it is crucial to address patients’ reservations early, conveying the understanding that psychological mechanisms do not contradict but complement biological ones and offer potential points of intervention on a behavioral level that may support the biological healing process.
The patient’s compliance with interventions is essential for successful treatment. This involves not only maintaining general motivation for therapy but also adhering to the behavioral adaptations elaborated to keep activities within the area of endurable load. For Protective Coping, this includes gradual activity increases, which may be challenging for patients with pronounced fears of overexertion. At the same time, for Active Coping, this involves to resist engaging in demanding activities, even when they may offer immediate rewards. To enhance compliance with our intervention, strategies such as Motivational Interviewing (MI) have potential benefits. MI has been shown to be effective in a wide range of psychological treatments (Bischof et al., 2021), in cases of skepticism toward psychotherapy (Tolchin et al., 2020), and in first studies including a post COVID sample (Leon-Herrera et al., 2024).
Our clinical experience primarily involves mildly to moderately affected fatigue patients and does not extend to patients severely affected by Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS), who experience profound impairments in daily functioning. Behavioral analysis as applied by our model requires detailed conversations, which severely impaired patients cannot sustain due to rapid fatigue and limited attention. The conversations can be not only cognitively but emotionally demanding, and even minimal physical load can worsen symptoms (Hartlieb, 2021) due to post-exertional malaise (PEM). Thus, the model’s applicability must be carefully evaluated and adapted for more severely affected individuals. Practical adaptations may, for example, include a reduction of session length, or providing online sessions to avoid overexertion by traveling.
In conclusion, our Model of Active and Protective Coping for Chronic Fatigue provides a new and comprehensive framework for individualized Cognitive Behavioral Therapy, considering the dynamic changes in behavioral coping patterns observed in chronic fatigue patients. By integrating both phases of coping and by addressing the complex interplay between them, this model offers added value for both therapy and research. We hope that it will serve as a foundation for more individualized and effective therapeutic interventions, ultimately improving the quality of care for patients suffering from chronic fatigue.
Data Availability
Data is provided within the manuscript.
Change history
14 May 2025
The anonymous version of the first supplementary file has been replaced with the complete file.
References
-
Al-Aly, Z., Davis, H., McCorkell, L., Soares, L., Wulf-Hanson, S., Iwasaki, A., & Topol, E. J. (2024). Long COVID science, research and policy. Nature Medicine, 30(8), 2148–2164. https://doi.org/10.1038/s41591-024-03173-6
-
Aschenbrenner, S., Kaiser, S., Pfüller, U., Roesch-Ely, D., & Weisbrod, M. (2012). Wiener Testsystem, Schuhfried.
-
Beck, A. T., Steer, R. A., & Brown, G. K. (2009). Beck-Depressions-Inventar (BDI–II, Dt. Version: M. Hautzinger, F. Keller & C. Kühner, 2. Aufl). Pearson Assessment.
-
Bierbauer, W., Lüscher, J., & Scholz, U. (2022). Illness perceptions in long-COVID: A cross-sectional analysis in adults. Cogent Psychology, 9(1). https://doi.org/10.1080/23311908.2022.2105007
-
Bischof, G., Bischof, A., & Rumpf, H. J. (2021). Motivational interviewing: An Evidence-Based approach for use in medical practice. Dtsch Arztebl Int, 118(7), 109–115. https://doi.org/10.3238/arztebl.m2021.0014
-
Bushnell, M. C., Ceko, M., & Low, L. A. (2013). Cognitive and emotional control of pain and its disruption in chronic pain. Nature Reviews Neuroscience, 14(7), 502–511. https://doi.org/10.1038/nrn3516
-
Davis, H. E., McCorkell, L., Vogel, J. M., & Topol, E. J. (2023). Long COVID: Major findings, mechanisms and recommendations. Nature Reviews Microbiology, 21(3), 133–146. https://doi.org/10.1038/s41579-022-00846-2
-
Engel, G. L. (1977). The need for A new medical model: A challenge for biomedicine. Science, 196(4286), 129–136. https://doi.org/10.1126/science.847460
-
Gaber, T. (2021). Assessment and management of post-COVID fatigue. Progress in Neurology and Psychiatry, 25(1), 36–39. https://doi.org/10.1002/pnp.698
-
Goudsmit, E. M., Nijs, J., Jason, L. A., & Wallman, K. E. (2012). Pacing as A strategy to improve energy management in myalgic encephalomyelitis/chronic fatigue syndrome: A consensus document. Disability and Rehabilitation, 34(13), 1140–1147. https://doi.org/10.3109/09638288.2011.635746
-
Grawe, K. (2004). Psychological therapy. Hogrefe & Huber.
-
Hartlieb, M. C. (2021). Psychotherapeutisch orientierte behandlungen beim chronic fatigue syndrome. Psychotherapie-Wissenschaft, 11(1), 51–56. https://doi.org/10.30820/1664-9583-2021-1-51
-
Hasting, A. S., Herzig, S., Obrig, H., Schroeter, M. L., Villringer, A., Thöne-Otto, A., & I., T. (2023). The Leipzig treatment program for interdisciplinary diagnosis and therapy of neurocognitive Post-COVID symptoms. Zeitschrift Für Neuropsychologie, 34(2), 71–83. https://doi.org/10.1024/1016-264X/a000376
-
Hayden, M. C. (2024). Impacts of COVID-19 on mental health. Zeitschrift Für Pneumologie. https://doi.org/10.1007/s10405-024-00562-z
-
Holtforth, M. G., & Grawe, K. (2000). Fragebogen Zur analyse motivationaler schemata (FAMOS). Zeitschrift Für Klinische Psychologie Und Psychotherapie, 29(3), 170–179. https://doi.org/10.1026//0084-5345.29.3.170
-
Holtzman, C. S., Bhatia, S., Cotler, J., & Jason, L. A. (2019). Assessment of Post-Exertional malaise (PEM) in patients with myalgic encephalomyelitis (ME) and chronic fatigue syndrome (CFS): A Patient-Driven survey. Diagnostics (Basel), 9(1). https://doi.org/10.3390/diagnostics9010026
-
Jason, L., Benton, M., Torres-Harding, S., & Muldowney, K. (2009). The impact of energy modulation on physical functioning and fatigue severity among patients with ME/CFS. Patient Education and Counseling, 77(2), 237–241. https://doi.org/10.1016/j.pec.2009.02.015
-
Kanfer, F. H., Reinecker, H., & Schmelzer, D. (2012). Self management therapy. A text book for clinical practice. Springer.
-
Koczulla, A. R., Ankermann, T., Behrends, U., Berlit, P., Brinkmann, F., Frank, U., Gloeckl, R., Gogoll, C., Häuser, W., Hohberger, B., Huber, G., Hummel, T., Köllner, V., Krause, S., Kronsbein, J., Maibaum, T., Mooren, F. C., Pecks, U., Peters, E. M., & Zwick, R. H. (2024). S1-Leitlinie Long/Post-COVID. https://register.awmf.org/de/leitlinien/detail/020-027
-
Köllner, V., Etzrodt, F., Kleinschmidt, J., & Kupferschmitt, A. (2022). Psychosomatische rehabilitation des Post-COVID-Syndroms. Ärztliche Psychotherapie, 17(3). https://doi.org/10.21706/aep-17-3
-
Lemogne, C., Gouraud, C., Pitron, V., & Ranque, B. (2023). Why the hypothesis of psychological mechanisms in long COVID is worth considering. Journal of Psychosomatic Research, 165, 111135. https://doi.org/10.1016/j.jpsychores.2022.111135
-
Leon-Herrera, S., Olivan-Blazquez, B., Samper-Pardo, M., Aguilar-Latorre, A., & Sanchez Arizcuren, R. (2024). Motivational interviewing as a tool to increase motivation and adherence to a long COVID telerehabilitation intervention: Secondary data analysis from a randomized clinical trial. Psychol Res Behav Manag, 17, 157–169. https://doi.org/10.2147/PRBM.S433950
-
Park, N. H., Kang, Y. E., Yoon, J. H., Ahn, Y. C., Lee, E. J., Park, B. J., & Son, C. G. (2024). Comparative study for fatigue prevalence in subjects with diseases: A systematic review and meta-analysis. Scientific Reports, 14(1), 23348. https://doi.org/10.1038/s41598-024-74683-z
-
Penner, I. K., Raselli, C., Stocklin, M., Opwis, K., Kappos, L., & Calabrese, P. (2009). The fatigue scale for motor and cognitive functions (FSMC): Validation of a new instrument to assess multiple sclerosis-related fatigue. Multiple Sclerosis (Houndmills, Basingstoke, England), 15(12), 1509–1517. https://doi.org/10.1177/1352458509348519
-
Peter, R. S., Nieters, A., Krausslich, H. G., Brockmann, S. O., Gopel, S., Kindle, G., Merle, U., Steinacker, J. M., Rothenbacher, D., Kern, W. V., & Group, E. P. S. (2022). Post-acute sequelae of covid-19 six to 12 months after infection: Population based study. Bmj, 379, e071050. https://doi.org/10.1136/bmj-2022-071050
-
Sachenbacher, S., Heimkes, F., Wunderlich, N., Grosse-Wentrup, F., Adorjan, K., Stubbe, H., Thomas, A., Nedeljkovic, A., & Ubleis, A. (2023). [Psychotherapeutic concept of the post-COVID outpatient clinic at the LMU hospital]. Der Nervenarzt, 94(7), 637–639. https://doi.org/10.1007/s00115-023-01501-8(Psychotherapeutisches Konzept der Post-COVID-Ambulanz des LMU-Klinikums.).
-
Schilling, T. M., Klein, J. F., Aschenbrenner, S., Drengner, A., Randerath, J., & Weisbrod, M. (2023). Durchführbarkeit und ergebnisse einer psychotherapeutischen gruppentherapie für patienten Mit fatigue Sowie emotionalen und kognitiven störungen in folge einer COVID-19-Erkrankung. Nervenheilkunde, 42(05), 263–272. https://doi.org/10.1055/a-1989-0926
-
Tempfli, M., & Randerath, J. (2022). Post-COVID fatigue: Proposed phasic model as guidance for individual psychotherapy. World Federation for Neurorehabilitation Congress.
-
Tolchin, B., Baslet, G., Martino, S., Suzuki, J., Blumenfeld, H., Hirsch, L. J., Altalib, H., & Dworetzky, B. A. (2020). Motivational interviewing techniques to improve psychotherapy adherence and outcomes for patients with psychogenic nonepileptic seizures. Journal of Neuropsychiatry and Clinical Neurosciences, 32(2), 125–131. https://doi.org/10.1176/appi.neuropsych.19020045
-
Walker, S., Goodfellow, H., Pookarnjanamorakot, P., Murray, E., Bindman, J., Blandford, A., Bradbury, K., Cooper, B., Hamilton, F. L., Hurst, J. R., Hylton, H., Linke, S., Pfeffer, P., Ricketts, W., Robson, C., Stevenson, F. A., Sunkersing, D., Wang, J., Gomes, M., & Collaboration, L. (2023). Impact of fatigue as the primary determinant of functional limitations among patients with post-COVID-19 syndrome: A cross-sectional observational study. British Medical Journal Open, 13(6), e069217. https://doi.org/10.1136/bmjopen-2022-069217
-
Wickham, H. (2016). ggplot2: Elegant graphics for data analysis. Springer-. https://ggplot2.tidyverse.org
-
Wurz, A., Culos-Reed, S. N., Franklin, K., DeMars, J., Wrightson, J. G., & Twomey, R. (2022). I feel like my body is broken: Exploring the experiences of people living with long COVID. Quality of Life Research, 31(12), 3339–3354. https://doi.org/10.1007/s11136-022-03176-1
-
Yoon, J. H., Park, N. H., Kang, Y. E., Ahn, Y. C., Lee, E. J., & Son, C. G. (2023). The demographic features of fatigue in the general population worldwide: A systematic review and meta-analysis. Front Public Health, 11, 1192121. https://doi.org/10.3389/fpubh.2023.1192121
-
Young, J. E. (2005). Young Schema questionnaire–Short form 3 (YSQ-S3). Cognitive Therapy Center.
Acknowledgements
This work was funded by the Ministry of Science, Research and Arts Baden-Württemberg, within the framework of the new special funding line for COVID-19, part of the measures to combat the SARS-CoV-2 coronavirus pandemic (“Sonderförderlinie COVID-19, Teil der Maßnahmen zur Bekämpfung der Coronavirus SARS-CoV-2-Pandemie”) in the field of medical research (grant number MWK33-7532-56).The study was approved by the Ethics committee of the University of Konstanz (21/2022). The participant gave written informed consent prior to participation. The study was conducted in accordance with the declaration of Helsinki.
Funding
Open Access funding enabled and organized by Projekt DEAL. This work by Tempfli & Randerath was funded by the Ministry of Science, Research and Arts Baden-Württemberg, within the framework of the new special funding line for COVID-19, part of the measures to combat the SARS-CoV-2 coronavirus pandemic (“Sonderförderlinie COVID-19, Teil der Maßnahmen zurBekämpfung der Coronavirus SARS-CoV-2-Pandemie”) in the field of medical research (grant number MWK33-7532-56).
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Electronic Supplementary Material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
Reprints and permissions
About this article
Cite this article
Tempfli, M., Randerath, J. The Concept of Active and Protective Coping for Individual Psychotherapy in Chronic Fatigue: an Example from Post COVID. J Contemp Psychother (2025). https://doi.org/10.1007/s10879-025-09669-7
- Accepted
- Published
- DOI https://doi.org/10.1007/s10879-025-09669-7
Keywords
- Post COVID
- Fatigue
- Psychotherapy
- Explanatory model