Article Content
Abstract
How therapists’ interoceptive accuracy or awareness affects the therapy process, and especially the therapeutic alliance, has not been previously studied. In this paper, data on objectively defined interoceptive accuracy and subjectively assessed interoceptive awareness were collected from forty Finnish psychotherapists. Interoceptive accuracy was measured with a heartbeat discrimination task and interoceptive awareness using the Multidimensional Assessment of Interoceptive Awareness, version 2, questionnaire. The therapists and their clients evaluated their experience of the alliance and provided written descriptions of each session in the study period. Using mixed methods, we then examined the associations between interoception and the therapeutic alliance and client wellbeing, as well as how psychotherapists used their internal bodily sensations as a source of information.
The key result of this study showed that the therapists’ interoceptive accuracy and awareness were positively correlated with their experience of the alliance. Through thematic analysis, we identified five sub-themes that illustrate how bodily sensations serve as a source of information for the psychotherapist. However, the therapists’ interoceptive accuracy or awareness were not associated with the clients’ experiences of alliance or their wellbeing.
In conclusion, a psychotherapist’s increased interoceptive accuracy and high level of interoceptive awareness enhance the therapist’s own experience of therapeutic alliance with the client. In addition, their increased awareness of internal bodily sensations also brings more elaborated information to the therapeutic process.
Similar content being viewed by others
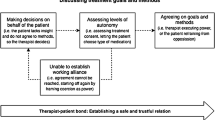
“It’s not a life of war and conflict”: experienced therapists’ views on negotiating a therapeutic alliance in involuntary treatment

Czech Version of the Multidimensional Assessment of Interoceptive Awareness (MAIA): Psychometric Evaluation and Network Model
Patient-Therapist Perspective of the Working Alliance in Psychotherapy
Explore related subjects
Discover the latest articles and news from researchers in related subjects, suggested using machine learning.
- Cognitive Behavioral Therapy
- Counseling Psychology
- Person-Centered Psychotherapy
- Psychodynamics
- Psychotherapy
- Therapeutic Relationship
Introduction
Recently, the field of psychotherapy research has seen a growing interest in how therapists’ interpersonal and intrapersonal qualities influence the therapeutic alliance (Clements-Hickman & Reese, 2023; Heinonen & Nissen-Lie, 2020). Initial studies have indicated that therapist characteristics have a stronger effect than patient characteristics in forming the therapeutic bond (Del Re et al., 2021). Furthermore, it has been suggested that therapists’ personality traits contribute to the alliance– and hence the therapy outcome– more than their age, gender, theoretical orientation, or clinical experience (Delgadillo et al., 2020; Wampold et al., 2017). Therapists’ abilities to be present and to attune to clients, their responsiveness, and their self-reflective skills are essential in achieving positive therapy outcomes (Wu & Levitt, 2022; Bennett-Levy, 2019). In addition, it has been suggested that therapists’ ability to access their own ongoing bodily sensations, helps them to adhere to their role as a therapist and make constructive use of their inner experience (Stange Bernhardt et al., 2021). Also, it has been demonstrated that a therapist’s bodily sensations change in interaction with the client during a therapy session (Chui & Hill, 2020).
The concept of interoception refers to the processing of signals originating from within the body and is used to describe the sensation and perception of these signals (Khalsa et al., 2018). Although the importance of bodily experiences is recognised, the role of interoception has so far received only minor attention in psychotherapy research. Previously, primarily the importance of differentiating between different dimensions of interoception has been emphasised. Interoceptive accuracy (IAcc) is defined as a trait-like variable linked to the ability to detect bodily signals such as heartbeats or hunger. IAcc can be assessed through objective behavioural tasks, which most often relate to the cardiovascular system (Pollatos & Herbert, 2018). Interoceptive awareness (IAw), on the other hand, is the subjective awareness of experienced bodily states and the ability to regulate them. IAw is most often assessed through self-report measures such as questionnaires or confidence ratings (Garfinkel et al., 2015).
As atypical interoception is associated with a risk for psychosomatic and psychiatric disorders (Brewer et al., 2021), it has mainly been studied in different patient groups. Poor interoception is linked, for example, to anxiety disorders (Yoris et al., 2015), schizophrenia (Torregrossa et al., 2022), eating disorders (Richard et al., 2019), and major depressive disorder (Eggart et al., 2019). However, interoceptive accuracy and awareness vary across all individuals and have received increasing attention as individual trait characteristics (Lyyra & Parviainen, 2018). Ovalle et al. (2023) found that therapists with higher interoceptive awareness reported greater warmth towards, and involvement with, their patients. In our earlier study, psychotherapists scored significantly higher on interoceptive awareness than their clients (Halonen et al., 2024). However, the interoceptive accuracy of the psychotherapists did not differ from that of a reference sample of individuals without therapeutic training. The present study seeks to further contribute to this line of research by investigating the associations between the therapists’ interoceptive accuracy (i.e., a physiological trait), interoceptive awareness (i.e., a subjective experience) and the therapeutic alliance. Hypothetically, a therapist with optimal interoceptive understanding will be sensitive to observing and interpreting their bodily sensations during a therapy session. Their autonomic nervous system reactions may attune with the client’s reactions, or they may consciously regulate their bodily reactions in a way that allows co-regulation of emotions with the client. This, in turn, is linked to the capability to foster a collaborative alliance and, thus, to the effectiveness of therapy.
The present study aligns with the central objective of the significant events research paradigm, which seeks to enhance our comprehension of change processes in psychotherapy by identifying the most beneficial events (Timulak, 2010). Certain significant events, such as moments of meeting, are frequently categorised as bodily experiences (Duarte et al., 2022). On the other hand, awareness of changes in bodily reactions can influence how therapists time their interventions during a session (Laitila et al., 2019). Furthermore, a change in bodily sensation can be a significant event for the client (Ladmanová et al., 2022). In change process research, it is important to commute between qualitative and quantitative methods to gain a more comprehensive understanding of the relationship between the phenomena under study (Faulkner, 2012).
Aim of the Study
In the present study, we investigate the potential associations between the interoception of psychotherapists and the therapeutic alliance. We study whether therapists’ interoceptive accuracy and/or awareness is associated with alliance ratings using quantitative methods. We also explore the associations of the aforementioned variables with clients’ well-being and interoceptive awareness. Further, we enrich the interoception–alliance connection by exploring how psychotherapists use their bodily sensations as a source of information in their clinical practice by utilising qualitative analysis.
Method
Participants
First, we collected data on interoception from 40 Finnish psychotherapists. Four therapists dropped out later for personal reasons, yielding a final sample of 36 therapists who collected data with 67 clients. The data covered a total of 651 therapy sessions. Of the 32 female and 4 male therapists, all were white Europeans. Their length of clinical experience as psychotherapists varied: 41.7% were trainees or had less than five years of clinical experience, 50% had five to fourteen years of experience, and 8.3% had 15 or more years of experience. The participating therapists represented different theoretical orientations: psychoanalytic or psychodynamic (11.1%), cognitive (27.8%), solution-focused (22.2%), integrative or cognitive-analytic (19.4%), trauma therapeutic (13.9%), and other (5.6%). It was emphasised to the clients that participation was voluntary and that refusal to participate would in no way affect the treatment they were receiving.
Procedure
The research design included a heartbeat discrimination task for each therapist at the outset of the study. An assessment of interoceptive awareness was carried out using a questionnaire for therapists and clients once at the beginning of the study period. They then reported, through questionnaires, their therapy process during 10 sessions. In most cases, the 10 sessions used for the study were part of longer therapies. The aim was to obtain a representative cross-section of psychotherapy in Finland, without limiting the data to a particular psychotherapy approach, phase of therapy, or patient group. Based on their clinical knowledge, therapists selected clients they considered suitable for the study– those willing and able to complete additional questionnaires– while ensuring that participation would not pose any risk, especially for vulnerable clients. The non-manualised therapy was conducted in a natural setting, and therapists were instructed to conduct their therapy processes in their usual manner. The research procedure was approved by the University of Jyväskylä Ethical Committee (1592/13.00.04.00/2020). All participants provided their written informed consent prior to participating in the research.
Interoceptive Accuracy
We selected the heartbeat discrimination task (HDT) for measuring interoceptive accuracy, i.e. the ability to detect bodily signals (Schandry, 1981). HDT is an established method for this purpose (Brener & Ring, 2016). The HDT in this study was modified to be used outside of a laboratory and adapted from the experimental procedure used at the Centre for Interdisciplinary Brain Research of the University Jyväskylä. The task included 16 one-minute observation periods with 30-second breaks between each period, 8 synchronised sets and 8 delayed sets in a randomised order. An ECG machine delivered synchronous tones 200 ms after the participant’s heartbeat. Asynchronous tones were delivered with an additional 300 ms delay. Immediately after each observation period, participants were asked whether they had perceived the tones to be synchronous or asynchronous with their heartbeat.
Interoceptive Awareness
The interoceptive awareness of both the clients and the therapists was assessed with the Multidimensional Assessment of Interoceptive Awareness, version 2 (MAIA-2) (Mehling et al., 2018). The MAIA questionnaire can be used to measure interoceptive awareness as a coherent construct (Ferentzi et al., 2021). Another important selection criterion for its use was that the questionnaire has been translated into Finnish and validated in the Finnish population (Kettunen & Kätkä, 2021).
The Therapeutic Alliance
The therapeutic alliance was monitored using the Session Rating Scale (SRS) at the end of each session (Duncan et al., 2003). The SRS comprises four visual analogue scales. Participants are asked to evaluate the therapeutic relationship, the relevance of the session topics, the suitability of the working method, and the overall session quality.
Client Wellbeing
The wellbeing of the clients and the progress of the therapy process were measured using the Outcome Rating Scale (ORS) at the beginning of each session (Bringhurst et al., 2006). The ORS comprises four visual analogue scales. Clients are asked to rate their individual wellbeing, wellbeing in close relationships, wellbeing in other social environments, and overall wellbeing.
Bodily Sensations as a Source of Information
The Helpful Aspects of Therapy (HAT) form has been developed for use in therapy change process research (Llewelyn, 1988). We translated the HAT into Finnish and abbreviated it so that its completion did not deduct too much time from the therapy session. We also added a question about bodily sensations, as we wanted information specifically on this issue. The HAT Finnish version contained four items: (1) “Of the events which occurred in this session, which one do you feel was the most important or helpful for you personally?”; (2) “Please describe what made this event important/helpful and what you got out of it. What observations did you make of your internal bodily sensations during the event?”; (3) “At about what point in the session did this event occur?”; (4) “Did anything happen during the session which might have hindered the therapy process? What kind of internal bodily sensations did you observe? At what point in the session did this event occur?”
Data Analysis
The quantitative data was analysed using IBM SPSS Statistics v28.0. Spearman’s correlations were performed to explore the associations between the therapists’ IAcc, the therapists’ and their clients’ IAw, SRS, and the clients’ ORS. This correlational analysis was conducted only for 31 therapists whose IAcc were measured successfully and who had collected the data with their clients. The data for the correlational analysis was aggregated as the therapists differed in their number of clients.
We chose to use reflective thematic analysis for the qualitative data to identify, describe, and interpret the patterns in it (Braun & Clarke, 2021). The method consists of six phases. Before embarking on the analysis, the first author transcribed all the therapists’ and clients’ HAT forms. This process generated an overall picture of the qualitative data.
- (1)Familiarisation: The first author conducted a preliminary coding to obtain an in-depth knowledge of the data.
- (2)Coding: After a discussion in a doctoral research seminar and with supervisors, all text in all the HAT forms containing references to shared bodily sensations and to the therapeutic alliance was extracted.
- (3)Generating initial themes: The first author sorted the extracts according to recurrent themes. At this point, due to the breadth of data, it was decided to focus on the use of internal bodily sensations as identified by the therapists. Initial themes were given tentative names.
- (4)Reviewing and developing themes: After a second data session, the first author re-read all the therapists’ HAT forms. She completed the preparation for pre-coding by double-checking that all the extracts focusing on the therapeutic alliance, shared bodily sensations, and use of bodily interventions were included. Thus, the unit of analysis to be coded was an extract from the therapist’s text that described a bodily sensation or bodywork. The next step in the analysis was a search for connections across the initial themes generated in phase 3.
- (5)Refining, defining, and naming themes: To ensure consistency in the coding process and to clarify the definitions of the themes, two psychology students were trained to code the data. The students’ codings were then compared and, in cases of disagreement, the extract was discussed by the three coders until a consensus was reached. The five final sub-themes, which comprised two clearly distinct main themes, were then refined and named.
- (6)Writing up: The two main themes and their five sub-themes were written up in the results section with authentic examples of the original extracts.
The Trustworthiness of the Qualitative Analysis
To enhance the trustworthiness of the qualitative analysis, we have, in accordance with the Lincoln-Guba framework, considered its credibility, transferability, dependability, confirmability, and authenticity. We have striven for credibility in the following ways. The first author has had prolonged engagement with the data while continually working with it from January 2022 to December 2023. Triangulation was used to ensure the consistency of the coding and to refine the definitions of the themes. Also, peer debriefers in doctoral research seminars helped to critically review the analysis. While the findings may not be transferable to other cultures or to all psychotherapy contexts, we consider them to be representative of current Finnish psychotherapists. To enhance dependability and ensure that the coding process was performed according to the descriptions of the themes, we used psychology students as co-coders. On the issue of confirmability, the first author’s interest in body-oriented psychotherapy has clearly influenced the research questions and primary analysis. Hence, to enhance objectivity, it was important that the other authors represented different perspectives on clinical psychology, psychotherapy, and neuropsychology. The authenticity of this study is demonstrated using direct quotations from the data.
Results
Descriptives
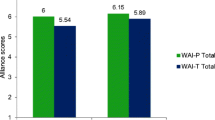
Client wellbeing was monitored with the Outcome Rating Scale. The overall ORS mean was 25.5 points, indicating that the clients in this sample primarily scored on the level typically associated with being a client (i.e., score below 25). The clients’ scores ranged from 9.6 to 36.5. This shows that our sample included both clients with severe mental health disorders and clients with milder psychological issues. The change in ORS ratings between the first and last therapy sessions varied significantly. During the research period, the greatest decrease in client wellbeing was 14.4 points, while the greatest increase was 25.7 points. This variation can be explained by the fact that these therapy processes are parts of long-term psychotherapy. On average, the alliance ratings of the clients in our sample were higher (M = 37.1) than those of therapists (M = 34.5). Conversely, the therapists gave higher ratings (M = 5.5) than their clients (M = 1.1) on the improvement in the alliance during the research period.
Quantitative Results
The correlational analysis showed three statistically significant associations, as shown in Table 1. The therapists’ interoceptive accuracy (r =.50, p =.005) and interoceptive awareness (r =.43, p =.017) were positively associated with their rating of the alliance. The clients’ interoceptive awareness was also positively associated with the clients’ ratings of the alliance (r =.50, p =.005). In other words, we found evidence that the participants’ interoception was related to their evaluation of the therapeutic alliance. Participants with higher interoceptive accuracy and awareness tended to evaluate the therapeutic alliance more positively. However, the therapists’ interoceptive accuracy and awareness were not associated with their clients’ experience of the alliance or their clients’ wellbeing.
Moreover, no correlation was observed between the therapists’ interoceptive accuracy and interoceptive awareness. This suggests that these are distinct dimensions of interoception, each warranting consideration as a separate variable in the study.
Qualitative Findings
During the familiarisation phase of the qualitative analysis, it became clear that the meanings and interpretations of bodily sensations were individual to each psychotherapist. For one therapist, an increase in alertness was a sign that he/she was on the verge of something important, whereas, for another therapist, it meant that he/she felt uncertain about what to do or say. Similarly, for one therapist, the feeling of bodily presence was a sign of gaining understanding, whereas, for another it indicated a strong alliance.
Conducting a thorough reflective thematic analysis yielded five sub-themes for how therapists used their internal bodily sensations. 90% of the therapists in this sample described bodily sensations in connection with the therapeutic alliance. Over half of the participating therapists consciously used the body as a tool in their psychotherapy sessions.
The first sub-theme, The body informs about the significance of the event, included descriptions of those moments when insight was gained or something new was discovered through the therapist’s bodily sensations. These perceptions were, thus, immediately connected to the topics of the session. Therapists described the events with words like insight, understanding, or voicing. Bodily sensations described by the therapist were, for example, release, warmth, and excitement.
Therapist 2: “Moment of client’s insight. Chills when we were at the core. Physical relief.”
In the second sub-theme, The therapeutic bond resonates in the body, bodily sensations were connected to the therapeutic alliance. Therapists either experienced a strong bond with the client or sensed a moment of disconnection. A moment of profound connection was described as synchrony, presence, or trust, whereas a moment of disconnection was described as restlessness, uncertainty, or frustration.
Therapist 4: “The connection is intimate, undisturbed, present, and supports co-operation. Sufficient calmness in the body when speaking, eye contact.”
or.
Therapist 24: “It’s hard to lead the conversation to more difficult issues, I’d like to focus only on nice, good things. I’m feeling restless and impatient. I am more motorically restless.”
The third sub-theme, The body as a tool, consisted of descriptions of the therapist’s active, conscious use of the body or bodily sensations as a tool in therapeutic work. These therapists used bodily techniques to self- or co-regulate emotions, verbally elaborated their own internal sensations, implemented bodily exercises, or used eye movement desensitisation and reprocessing.
Therapist 18: “The client talked about an emotion that she can’t grasp and can’t put into words. Through bodywork, we recognised that she was angry. Taking a pose helped to find a word for the feeling.”
The fourth sub-theme, Noticing bodily sensations, included bodily perceptions that were, for example, observations of the therapist’s state of alertness or awareness of uncomfortable, neutral, or comfortable bodily sensations.
Therapist 10: “My body was not alive and resonating today, so the work for my part happened more at the verbal level.”
In the fifth sub-theme, Emotional awareness, the therapist was aware of the connection between bodily sensations and emotional states or described emotional contagion without gaining insight through it. These descriptions pointed to therapists paying attention to bodily sensations and their connection with emotional states but did not always immediately link them to the topics raised in the session.
Therapist 12: “For a moment the client can experience irritation, and I felt it in my body as well, my stomach clenched.”
These five sub-themes can be divided into two main themes. When it comes to the first main theme, the therapist’s bodily sensations included bodily knowledge that had an immediate recognised effect on the therapy session or process. The first main theme contained the first three sub-themes described above. For the second main theme, bodily sensations were described as bodily information with no formulated meaning related to the therapy process at the time of the event. This second main theme contained the fourth and fifth sub-themes as previously described. Finding the second main theme suggests that therapists may register these bodily sensations because they understand that their meaning may only become apparent to them later in the therapeutic process. It is also possible that the therapist has an intuitive understanding that the client’s bodily sensation differs from his/her own.
Discussion
The overall aim of this study was to examine the relationship between interoception and the therapeutic alliance using quantitative and qualitative methods. In the statistical analysis we found that psychotherapists’ interoceptive accuracy and awareness were positively associated with their experience of the alliance. Nevertheless, therapists’ interoceptive accuracy or awareness was not related to their clients’ experience of the alliance or their clients’ well-being. It’s noteworthy that a positive association was also observed between clients’ interoceptive awareness and their own experience of the alliance. In order to align the results more closely with clinical work, we wanted to carry out a qualitative analysis and give meaning to the quantitative analysis. The primary outcome of the thematic analysis was the identification of how the therapists utilised their internal bodily sensations as a source of information. The following five sub-themes were identified: the body informs about the significance of the event; the therapeutic bond resonates in the body; the body as a tool; noticing bodily sensations; and emotional awareness. The therapists’ descriptions revealed that they actively paid attention to bodily sensations connected to the therapeutic alliance during significant events.
Interoception as a Characteristic of a Psychotherapist
We found that both dimensions of interoception, namely objectively defined interoceptive accuracy and subjectively assessed interoceptive awareness, were associated with a positive experience of the alliance. The hypothesis was formulated that a therapist with optimal interoceptive understanding would demonstrate sensitivity and the capability to cultivate a collaborative relationship. However, the measures selected for this study did not allow for the demonstration of a correlation between the therapist’s interoception and the client’s experience of the alliance or their wellbeing. Consequently, our hypothesis was only partially proven. The connection was found within-person but not between-persons.
Here, it is important to be clear on whether interoception is treated as a physiological trait or as a subjective experience. In this pioneering study, we attempted to assess both aspects. Firstly, it is important to note that our results did not demonstrate a correlation between interoceptive accuracy and awareness. These findings suggest that the relationship between interoception and alliance may be due to different underlying mechanisms when interoception is approached as a physiological tendency to be sensitive to bodily signals versus a self-assessed attribute.
Interestingly, interoceptive accuracy, when considered as an objectively measurable trait, is more closely associated with behavioural inhibition or the tendency to avoid aversive outcomes (Lyyra & Parviainen, 2018). This is in line with the reported association between, for example, interoception and anxiety (Yoris et al., 2015) and highlights that this concept should not be viewed as a mere skill but rather as an inherent tendency or trait of the individual that can confer benefits for therapists but also predispose them to adverse outcomes (Haase et al., 2016; Schultchen et al., 2019).
The role of the therapist’s interoception in psychotherapy research has, thus far, been relatively under-examined. To the best of our knowledge, Ovalle’s (2023) and the present study are the only ones that have focused on psychotherapists’ interoception. However, it may be that increased awareness of the body’s internal sensations and the ability to recognise and regulate bodily reactions can help therapists in their therapeutic interaction (Sands, 2023). Previous research also implies that individuals with better interoception are better able to form connections with others (Heydrich et al., 2021). Therefore, developing interoceptive awareness may help both therapists and clients and, thus, indirectly affect the experience of the alliance.
Since objectively measured interoceptive accuracy and subjective interoceptive awareness were related to the alliance, these initial findings support the idea that interoception is one of the characteristics of a psychotherapist that merits further investigation. Interoception indicates the state of the autonomic nervous system and previous research has indicated that physiological synchrony of the autonomic nervous system is related to alliance evaluations in psychotherapy (Tourunen et al., 2020; Tschacher & Meier, 2020). Therefore, it seems reasonable to suggest that this new information will build on that research. Furthermore, the study illuminates the understanding of therapy from the perspective of therapists themselves, as well as the factors that may render them susceptible to, or resilient against, the psychological strain associated with therapy work (Van Hoy & Rzeszutek, 2022).
Internal Bodily Sensations as an Information Source
In terms of clinical work and psychotherapy training, our study provides information on the variety of ways in which therapists use bodily sensations as a source of information. The influence of bodily sensations on therapeutic interaction is a phenomenon that is present regardless of whether psychotherapists are aware of it or not (Tschacher & Pfammatter, 2016). In psychotherapy, bodily sensations should be approached with an open mind and explorative attitude, just like thoughts and emotions. Without conscious attention to bodily sensations, therapists may overlook the client’s experience of the alliance or miss opportunities for deeper exploration. Cultivating bodily awareness, therefore, is a valuable tool in strengthening the therapeutic process (Sletvold, 2016; Price & Weng, 2021). Surprisingly, the therapists in this study not only reported observations related immediately to the topics of the session but also their observations of other bodily sensations, the significance of which they had not yet determined. It may be that therapists are becoming more attuned to these phenomena knowing that, as more information accumulates, they may have relevance for the therapy process. Whilst it can be argued that bodily sensations may possess a more generalised significance, it is important to acknowledge that, within the individual, such sensations can hold distinct and unique connotations for both the therapist and the client.
Our study confirmed previous findings on psychotherapists’ somatic experiences (Shaw, 2004), and it complemented these by identifying the second main theme, Bodily information for which no meaning related to the therapy process had been formulated at the time. In Shaw’s (2004) grounded theory-based paper, a theme called Body as a receiver reported observations that something was being bodily communicated to the therapists. This resembles our sub-theme The body informs about the significance of the event. Shaw’s theme Body empathy is similar to the sub-theme The therapeutic bond resonates in the body. Shaw’s theme Body management refers to styles and techniques and was structured in the same way as our sub-theme The body as a tool. Despite their different research methods, very similar themes were found in the data sets in these two studies.
Limitations and Future Directions
The two phenomena under investigation, namely interoception and alliance, are both complex in nature. The participants involved in the study displayed a range of experiences, as well as a diversity of interpretations regarding the meanings attributed to these experiences. The observed lack of relationship between the therapist’s interoceptive accuracy or awareness and the effectiveness of therapy in this study may be attributable to the fact that our research design which was mainly based on questionnaires did not achieve the requisite levels of embodied interaction, particularly regarding its long-term implications.
This study was limited by the relatively small sample of therapists available. In addition, these therapists’ interest in participating in this study may indicate that they were more aware of embodiment in psychotherapy than therapists on average. Also, the Hawthorne effect may have had an impact on the results. However, the data was collected from 651 therapy sessions, which can be considered a representative sample in a single psychotherapy study. Representativeness was also increased by the fact that our therapists had different theoretical orientations and varying lengths of clinical experience.
Further research might explore whether the association between interoceptive accuracy or awareness and the alliance is related to a better ability by the therapist to distinguish between which sensations are their own and which are related to the therapeutic interaction or to the client. This also prompts the question of how the therapist distinguishes them and what informs the distinctions of which are their own sensations, which they mirror from the clients, and which are related to the quality of interaction. More research is also required to gain a deeper understanding of the role of interoceptive accuracy as a trait-like characteristic in embodied interaction and bodily synchrony.
Conclusion
These findings shed new light on therapists’ use of bodily sensations in assessing the therapeutic alliance. Intriguingly, both interoceptive accuracy and awareness were found to be related to the psychotherapist’s rating of their experience of alliance. On one hand, further research is required to ascertain whether interoceptive accuracy is associated with the therapist’s autonomic nervous system’s reactivity in therapeutic settings and its implications for the therapist’s wellbeing. On the other hand, we need evidence on whether the therapist can promote a more positive alliance by developing both his or her own, as well as the client’s, interoceptive awareness, thus, increasing the effectiveness of therapy. Despite the exploratory nature of our study, we consider that these results strengthen the bodily perspective in psychotherapy and hope that they will inspire both clinicians and researchers. Our objective was to increase the understanding of interoception as one of the characteristics of a psychotherapist, and the present study demonstrated that internal bodily sensations and the underlying interoception are relevant to how the participants experienced the alliance.
Data Availability
No datasets were generated or analysed during the current study.
References
-
Bennett-Levy, J. (2019). Why therapists should walk the talk: The theoretical and empirical case for personal practice in therapist training and professional development. Journal of Behavior Therapy and Experimental Psychiatry, 62, 133–145. https://doi.org/10.1016/j.jbtep.2018.08.004
-
Braun, V., & Clarke, V. (2021). Can I use TA? Should I use TA? Should I not use TA? Comparing reflexive thematic analysis and other pattern-based qualitative analytic approaches. Counselling and Psychotherapy Research, 21(1), 37–47. https://doi.org/10.1002/capr.12360
-
Brener, J., & Ring, C. (2016). Towards a psychophysics of interoceptive processes: The measurement of heartbeat detection. Phil Trans R Soc B, 371, 20160015. https://doi.org/10.1098/rstb.2016.0015
-
Brewer, R., Murphy, J., & Bird, G. (2021). Atypical interoception as a common risk factor for psychopathology: A review. Neuroscience & Biobehavioral Reviews, 130, 470–508. https://doi.org/10.1016/j.neubiorev.2021.07.036
-
Bringhurst, D., Watson, C., Miller, S., & Duncan, B. (2006). The reliability and validity of the outcome rating scale: A replication study of a brief clinical measure. Journal of Brief Therapy, 5(1), 23–30.
-
Chui, H., & Hill, C. (2020). Keep calm and alert and carry on: Therapist calmness and fatigue in relation to session process. Counselling Psychology Quarterly, 33(1), 66–78. https://doi.org/10.1080/09515070.2018.1502160
-
Clements-Hickman, A., & Reese, R. (2023). The person of the therapist: Therapists’ personal characteristics as predictors of alliance and treatment outcomes. Psychotherapy Research, 33(2), 173–184. https://doi.org/10.1080/10503307.2022.2080610
-
Del Re, A., Flückiger, C., Horvath, A., & Wampold, B. (2021). Examining therapist effects in the alliance-outcome relationship: A multilevel meta-analysis. Journal of Consulting and Clinical Psychology, 89(5), 371–378. https://doi.org/10.1037/ccp0000637
-
Delgadillo, J., Branson, A., Kellett, S., Myles-Hooton, P., Hardy, G., & Shafran, R. (2020). Therapist personality traits as predictors of psychological treatment outcomes. Psychotherapy Research, 30(7), 857–870. https://doi.org/10.1080/10503307.2020.1731927
-
Duarte, J., Martinez, C., & Tomicic, A. (2022). Sparks of psychotherapeutic change: How therapists understand moments of meetings’ contribution to change in psychotherapy. Psychotherapy Research, 32(4), 511–524. https://doi.org/10.1080/10503307.2021.1948138
-
Duncan, B., Miller, S., Sparks, J., Claud, D., Reynolds, L., Brown, J., & Johnson, L. (2003). The session rating scale: Preliminary psychometric properties of a ‘working’ alliance measure. Journal of Brief Therapy, 3, 3–12.
-
Eggart, M., Lange, A., Binser, M., Queri, S., & Müller-Oerlinghausen, B. (2019). Major depressive disorder is associated with impaired interoceptive accuracy: A systematic review. Brain Sciences, 9(6). https://doi.org/10.3390/brainsci9060131. Article 131.
-
Faulkner, A. (2012). Participation and service user involvement. In D. Harper, & A. Thompson (Eds.), Qualitative research methods in mental health and psychotherapy: A guide for students and practitioners (pp. 39–54). Wiley-Blackwell.
-
Ferentzi, E., Olaru, G., Geiger, M., Vig, L., Köteles, F., & Wilhelm, O. (2021). Examining the factor structure and validity of the multidimensional assessment of interoceptive awareness. Journal of Personality Assessment, 103(5), 675–684. https://doi.org/10.1080/00223891.2020.1813147
-
Garfinkel, S., Seth, A., Barrett, A., Suzuki, K., & Critchley, H. (2015). Knowing your own heart: Distinguishing interoceptive accuracy from interoceptive awareness. Biological Psychology, 104, 65–74. https://doi.org/10.1016/j.biopsycho.2014.11.004
-
Haase, L., Stewart, J., Youssef, B., May, A., Isakovic, S., Simmons, A., Johnson, D., Potterat, E., & Paulus, M. (2016). When the brain does not adequately feel the body: Links between low resilience and interoception. Biological Psychology, 113, 37–45. https://doi.org/10.1016/j.biopsycho.2015.11.004 [anonymized for peer review].
-
Halonen, S., Laitila, A., Parviainen, T., & Kykyri, V-L. (2024). Psychotherapists’ interoceptive awareness and accuracy. Counselling and Psychotherapy Research, Early View. https://doi.org/10.1002/capr.12864
-
Heinonen, E., & Nissen-Lie, H. (2020). The professional and personal characteristics of effective psychotherapists: A systematic review. Psychotherapy Research, 30(4), 417–432. https://doi.org/10.1080/10503307.2019.1620366
-
Heydrich, L., Walker, F., Blättler, L., Herbelin, B., Blanke, O., & Aspell, J. (2021). Interoception and empathy impact perspective taking. Frontiers in Psychology, 11, 599429. https://doi.org/10.3389/fpsyg.2020.599429
-
Kettunen, P., & Kätkä, K. (2021). Suomenkielisen MAIA-2–mittarin validointitutkimus yleisväestöaineistolla [The validation study of Finnish MAIA-2] [Master’s Thesis, University of Eastern Finland]. https://erepo.uef.fi/handle/123456789/25107
-
Khalsa, S., Adolphs, R., Cameron, O., Critchley, H., Davenport, P., Feinstein, J., Feusner, J., Garfinkel, S., Lane, R., Mehling, W., Meuret, A., Nemeroff, C., Oppenheimer, S., Petzschner, F., Pollatos, O., Rhudy, J., Schramm, L., Simmons, W., & Stein, M. (2018). Interoception and mental health: A roadmap. Biological Psychiatry-Cognitive Neuroscience and Neuroimaging, 3(6), 501–513. https://doi.org/10.1016/j.bpsc.2017.12.004.… and the Interoception Summit 2016 participants.
-
Ladmanová, M., Řiháček, T., & Ladislav, T. (2022). Client identified impacts of helpful and hindering events in psychotherapy: A qualitative Meta-analysis. Psychotherapy Research, 32(6), 723–735. https://doi.org/10.1080/10503307.2021.2003885
-
Laitila, A., Vall, B., Penttonen, M., Karvonen, A., Kykyri, V.-L., Tsatsishvili, V., Kaartinen, J., & Seikkula, J. (2019). The added value of studying embodied responses in couple therapy research: A case study. Family Process, 58 (3),685–697. https://doi.org/10.1111/famp.12374
-
Llewelyn, S. (1988). Psychological therapy as used by clients and therapists. The British Journal of Clinical Psychology / the British Psychological Society, 27 (Pt(3), 223–237. https://doi.org/10.1111/j.2044-8260.1988.tb00779.x
-
Lyyra, P., & Parviainen, T. (2018). Behavioural inhibition underlies the link between interoceptive sensitivity and anxiety-related temperamental traits. Frontiers in Psychology, 9. https://www.frontiersin.org/articles/10.3389/fpsyg.2018.01026
-
Mehling, W., Acree, M., Stewart, A., Silas, J., & Jones, A. (2018). The multidimensional assessment of interoceptive awareness, version 2 (MAIA-2). PLOS ONE, 13(12), e0208034. https://doi.org/10.1371/journal.pone.0208034
-
Ovalle, A., Fischer, C., Dagnino, P., & Vaccarezza, S. (2023). Interoceptive awareness and therapist characteristics. Counselling and Psychotherapy Research, 00, 1–10. https://doi.org/10.1002/capr.12701
-
Pollatos, O., & Herbert, B. (2018). Interoception: Definitions, dimensions, neural substrates. In G. Hauke, & A. Kritikos (Eds.), Embodiment in psychotherapy, A practioners guide (pp. 15–27). Springer.
-
Price, C., & Weng, H. (2021). Facilitating adaptive emotion processing and somatic reappraisal via sustained mindful interoceptive attention. Frontiers of Psychology 12:578827. https://doi.org/10.3389/fpsyg.2021.578827
-
Richard, A., Meule, A., Georgii, C., Voderholzer, U., Cuntz, U., Wilhelm, F., & Blechert, J. (2019). Associations between interoceptive sensitivity, intuitive eating, and body mass index in patients with anorexia nervosa and normal-weight controls. European Eating Disorders Review: the Journal of the Eating Disorders Association, 27(5), 571–577. https://doi.org/10.1002/erv.2676
-
Sands, S. (2023). Inside the body: How the science of interoception can provide a new Understanding of psychoanalysis. Psychoanalytic Dialogues, 33(2), 267–277. https://doi.org/10.1080/10481885.2023.2173971
-
Schandry, R. (1981). Heartbeat perception and emotional experience. Psychophysiology, 18(4), 483–488. https://doi.org/10.1111/j.1469-8986.1981.tb02486.x
-
Schultchen, D., Bayer, J., Kühnel, J., Melchers, K., & Pollatos, O. (2019). Interoceptive accuracy is related to long-term stress via self‐regulation. Psychophysiology, 56(10), Article13429. https://doi.org/10.1111/psyp.13429
-
Shaw, R. (2004). The embodied psychotherapist: An exploration of the therapists’ somatic phenomena within the therapeutic encounter. Psychotherapy Research, 14(3), 271–288. https://doi.org/10.1093/ptr/kph025
-
Sletvold, J. (2016). The analyst’s body: A relational perspective from the body. Psychoanalytic Perspectives, 13(2), 186–200. https://doi.org/10.1080/1551806X.2016.1156433
-
Stange Bernhardt, I., Nissen-Lie, H., & Råbu, M. (2021). The embodied listener: A dyadic case study of how therapist and patient reflect on the significance of therapist’s personal presence for the therapeutic change process. Psychotherapy Research, 31(5), 682–694. https://doi.org/10.1080/10503307.2020.1808728
-
Timulak, L. (2010). Significant events in psychotherapy: An update of research findings. Psychology and Psychotherapy: Theory Research and Practice, 83(4), 421–447. https://doi.org/10.1348/147608310X499404
-
Torregrossa, L., Amedy, A., Roig, J., Prada, A., & Park, S. (2022). Interoceptive functioning in schizophrenia and schizotypy. Schizophrenia Research, 239, 151–159. https://doi.org/10.1016/j.schres.2021.11.046
-
Tourunen, A., Kykyri, V-L., Seikkula, J., Kaartinen, J., Tolvanen, A., & Penttonen, M. (2020). Sympathetic nervous system synchrony: An exploratory study of its relationship with the therapeutic alliance and outcome in couple therapy. Psychotherapy, 57, 160–173. https://doi.org/10.1037/pst0000198
-
Tschacher, W., & Meier, D. (2020). Physiological synchrony in psychotherapy sessions. Psychotherapy Research, 30(5), 558–573. https://doi.org/10.1080/10503307.2019.1612114
-
Tschacher, W., & Pfammatter, M. (2016). Embodiment in psychotherapy—A necessary complement to the canon of common factors? European Psychotherapy, 2016/2017, 9–25.
-
Van Hoy, A., & Rzeszutek, M. (2022). Burnout and psychological wellbeing among psychotherapists: A systematic review. Frontiers in Psychology, 13., Article 928191. https://doi.org/10.3389/fpsyg.2022.928191
-
Wampold, B., Baldwin, S., Holtforth, M., & Imel, Z. (2017). What characterizes effective therapists? In L. Castonguay & C. Hill (Eds.), How and why are some therapists better than others? Understanding therapist effects (37–53). American Psychological Association. https://doi.org/10.1037/0000034-003
-
Wu, M., & Levitt, H. (2022). How to become a responsive therapist: A study of experiences of developing therapists. Psychotherapy Research, 32(6), 763–777. https://doi.org/10.1080/10503307.2021.2009929
-
Yoris, A., Esteves, S., Couto, B., Melloni, M., Kichic, R., Cetkovich, M., Favaloro, R., Moser, J., Manes, F., Ibanez, A., & Sedeño, L. (2015). The roles of interoceptive sensitivity and metacognitive interoception in panic. Behavioral and Brain Functions, 11(1). https://doi.org/10.1186/s12993-015-0058-8
Acknowledgements
We thank Viki-Veikko Elomaa for technical support with the heartbeat discrimination device and Joona Muotka for statistical advice. Special thanks go to the therapists and their clients who participated in the study.
Funding
Open Access funding provided by University of Jyväskylä (JYU).
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
Reprints and permissions
About this article
Cite this article
Halonen, S., Laitila, A., Parviainen, T. et al. The Role of the Psychotherapist’s Interoception in the Therapeutic Alliance. J Contemp Psychother (2025). https://doi.org/10.1007/s10879-025-09681-x
- Accepted
- Published
- DOI https://doi.org/10.1007/s10879-025-09681-x
Keywords
- Alliance
- Psychotherapist
- Interoception
- Embodiment
- Significant Events